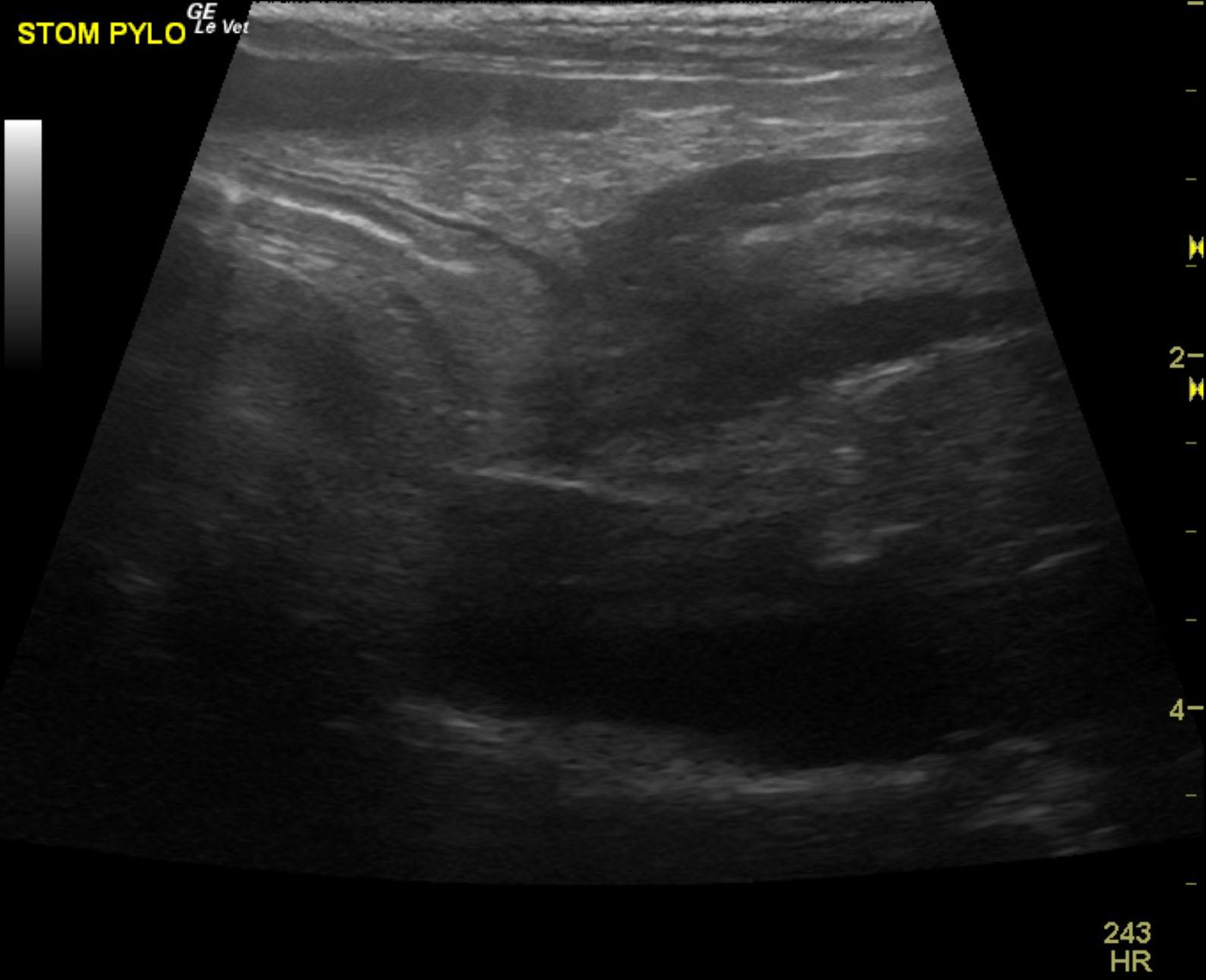
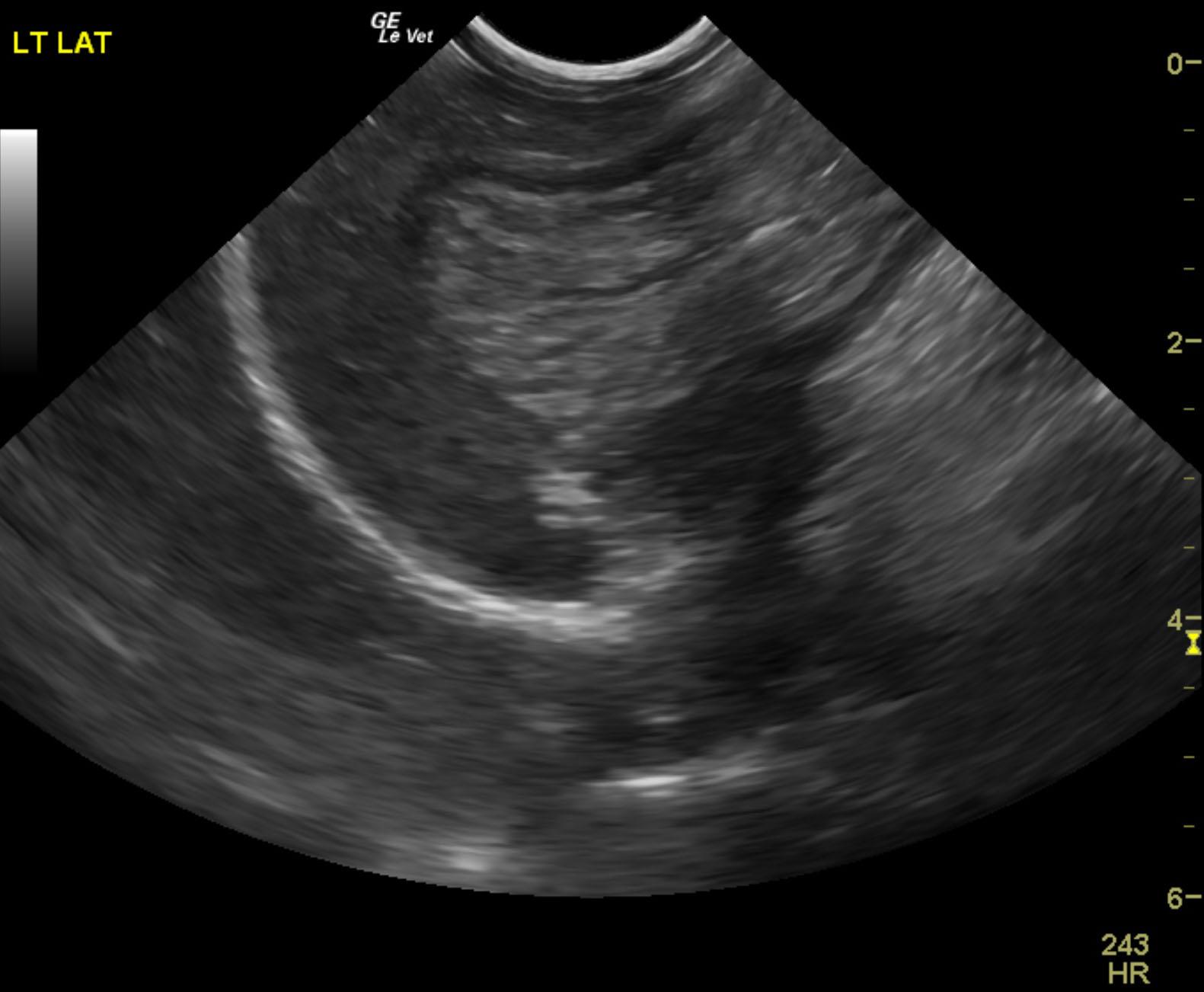
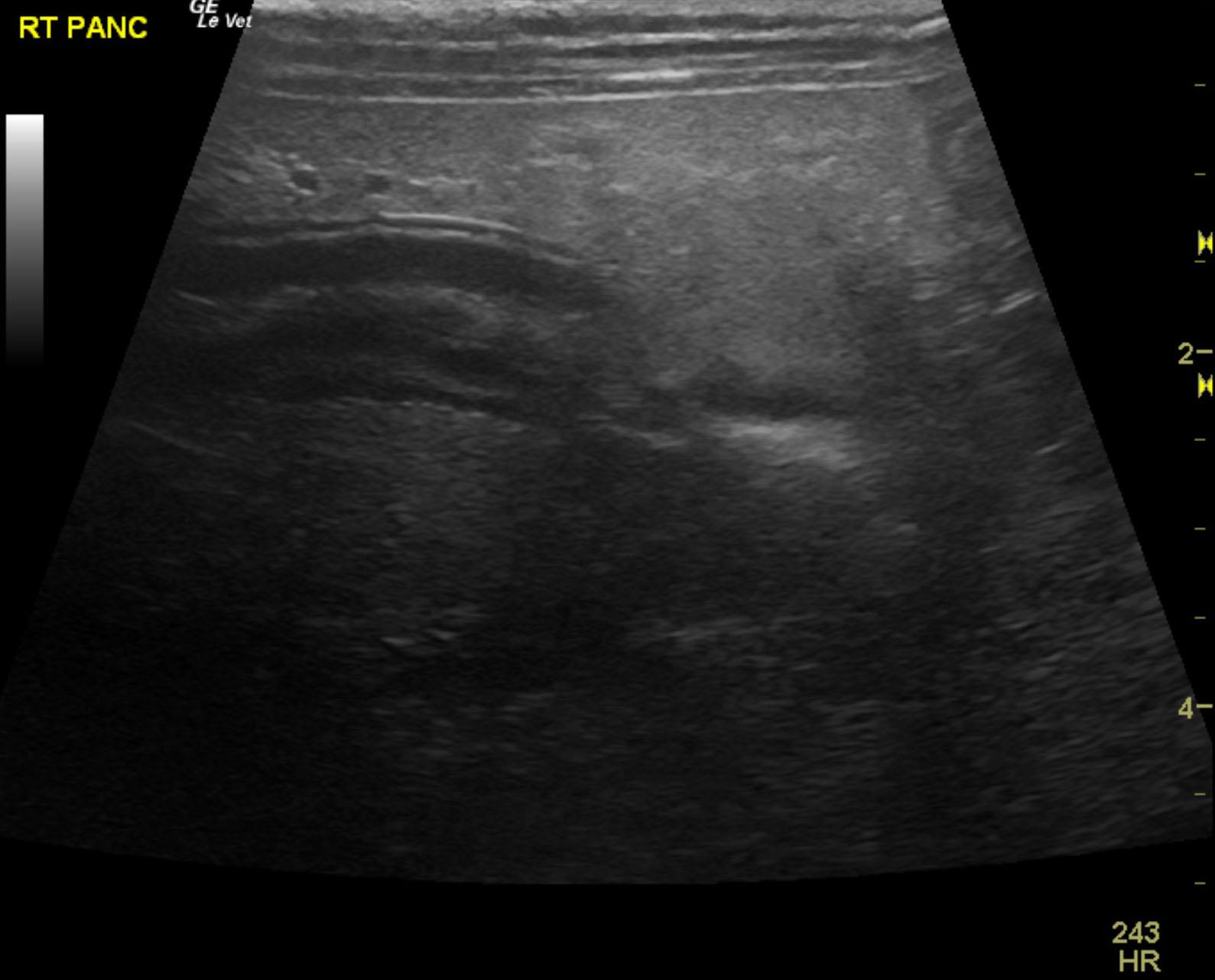
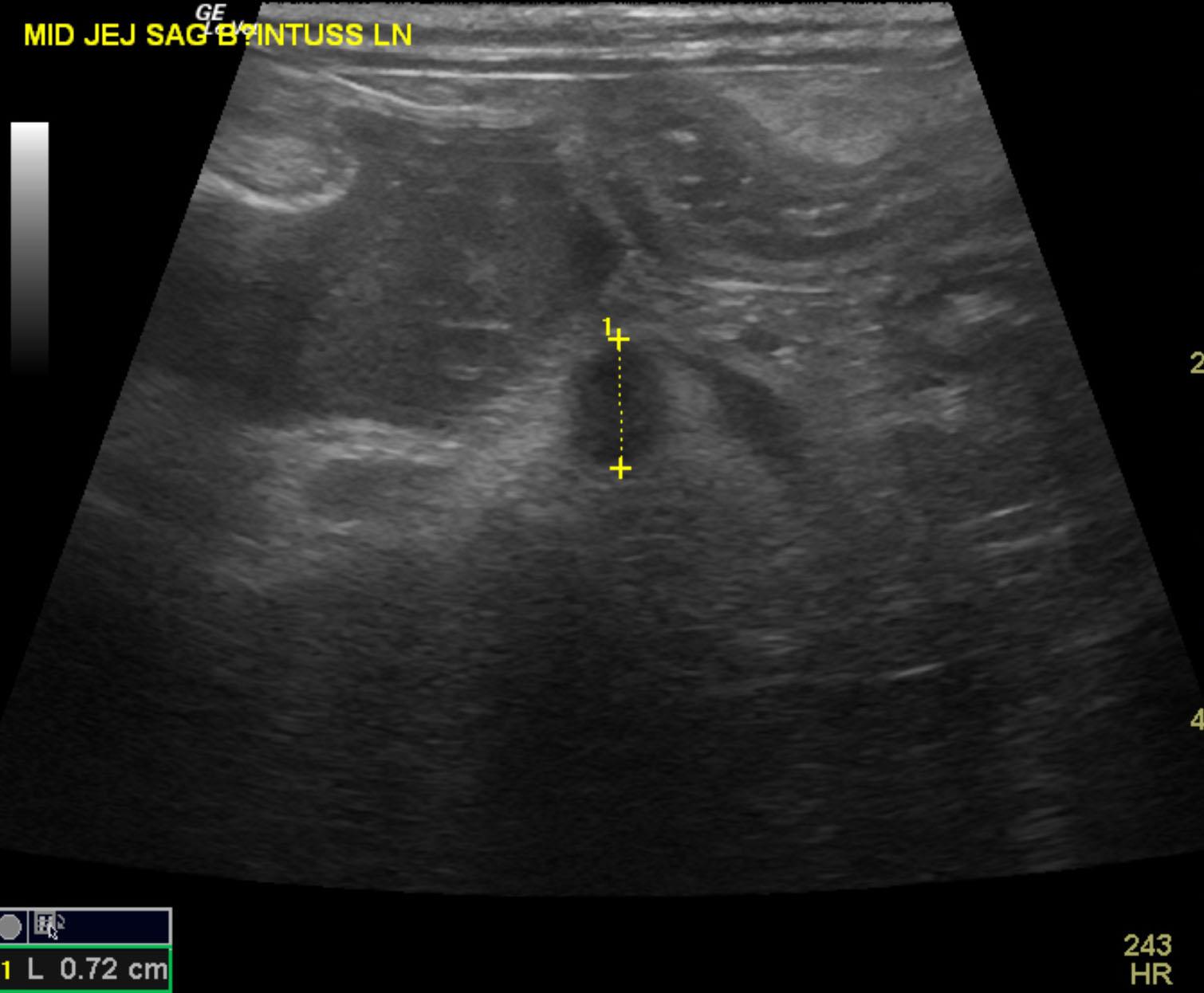
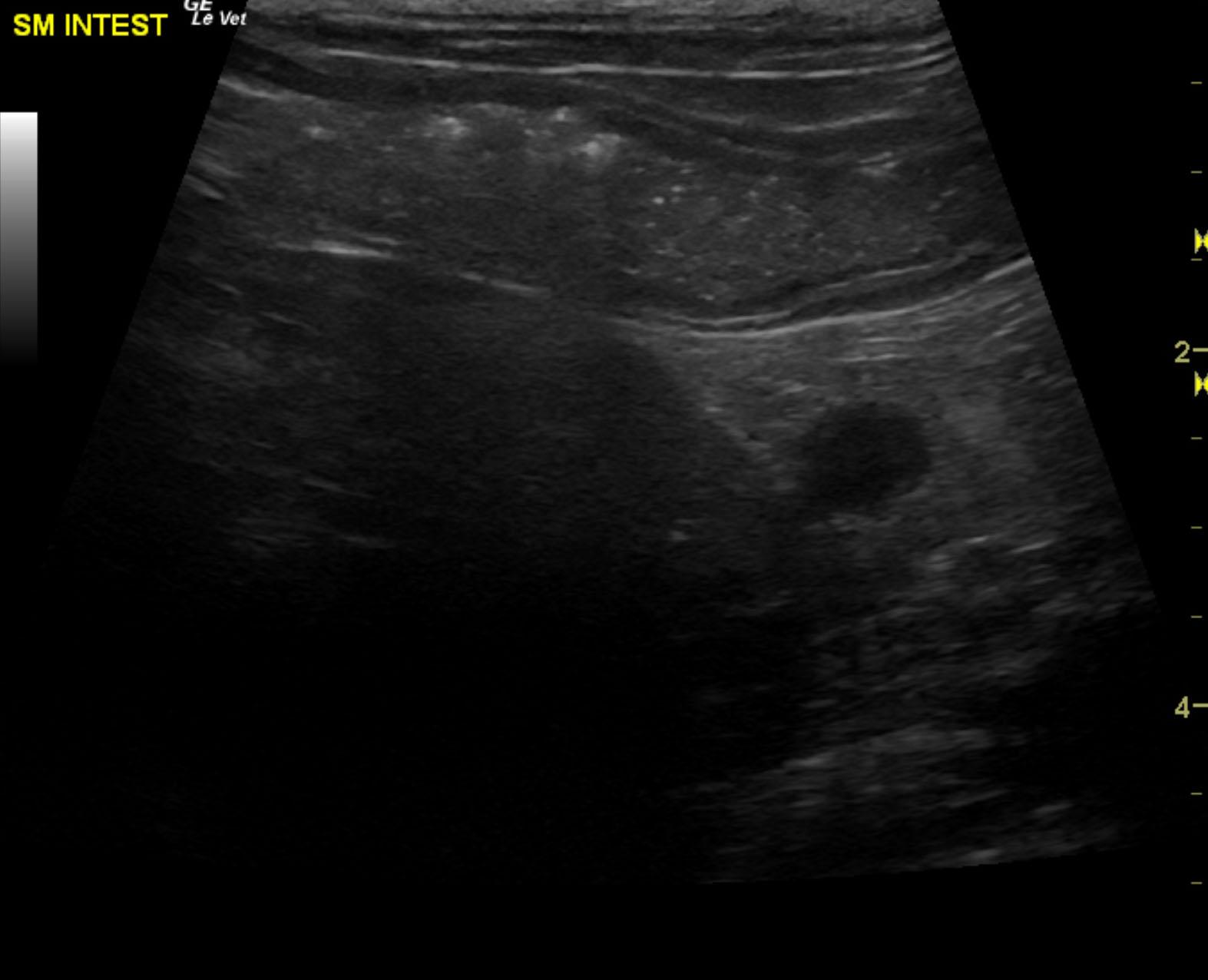
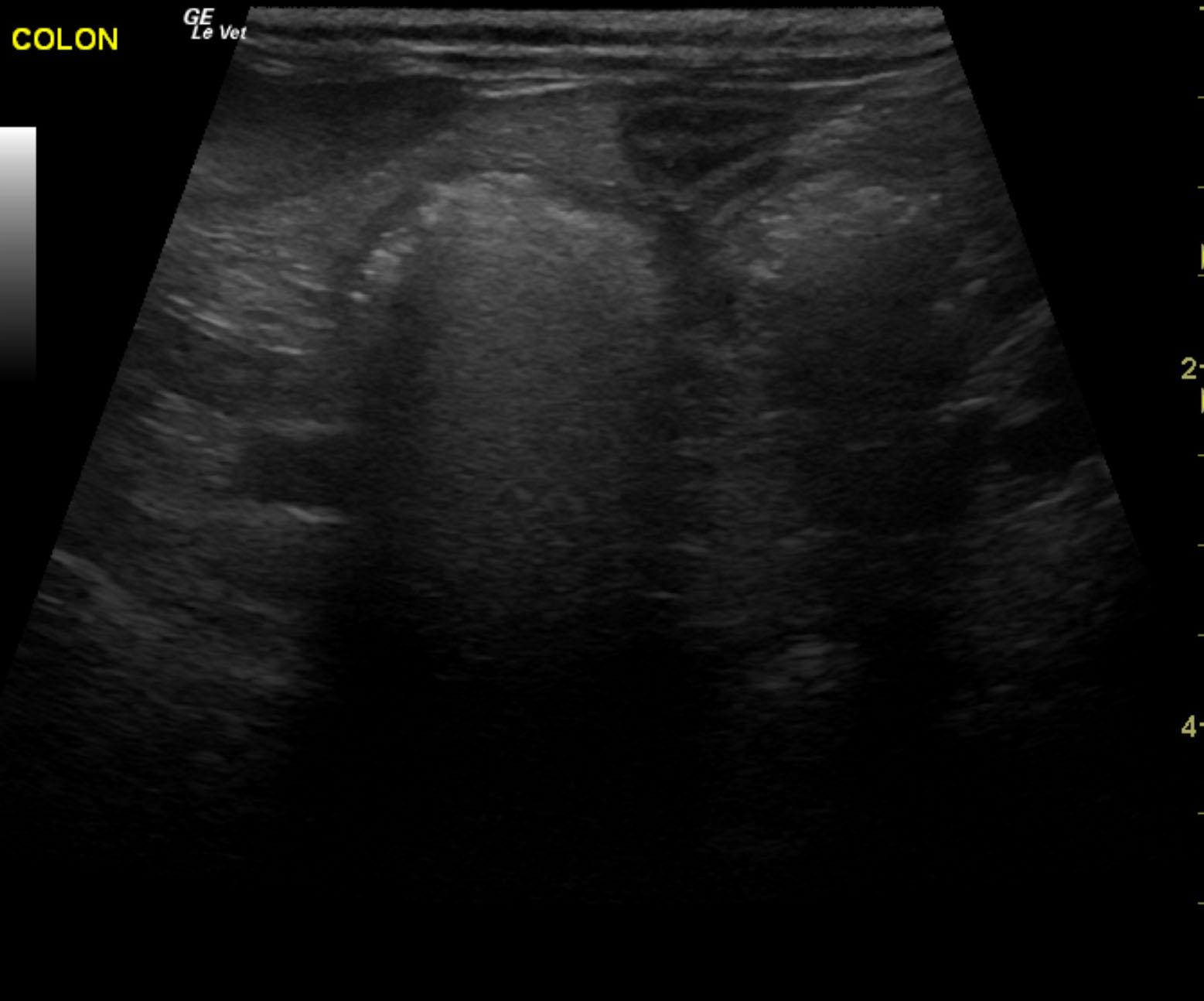
The patient is a 13 year old spayed female Dachshund dog which was presented for four days of anorexia and vomiting. She was given Cerenia, which helped, but still had ileus. Dog has vomited carpet material in past. Spec cPL was normal. Radiographs revealed dilated intestine, which appeared to be colon and cecum.