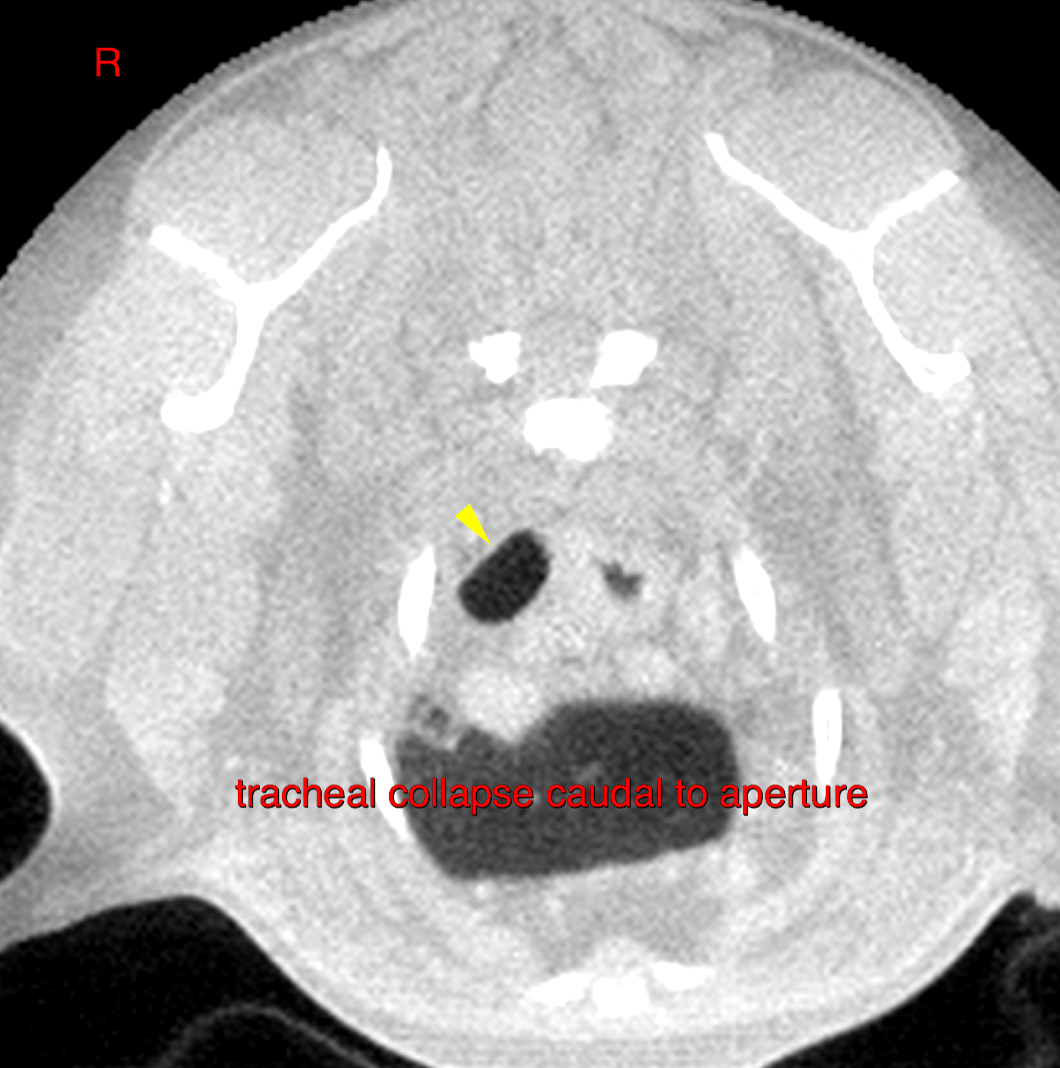
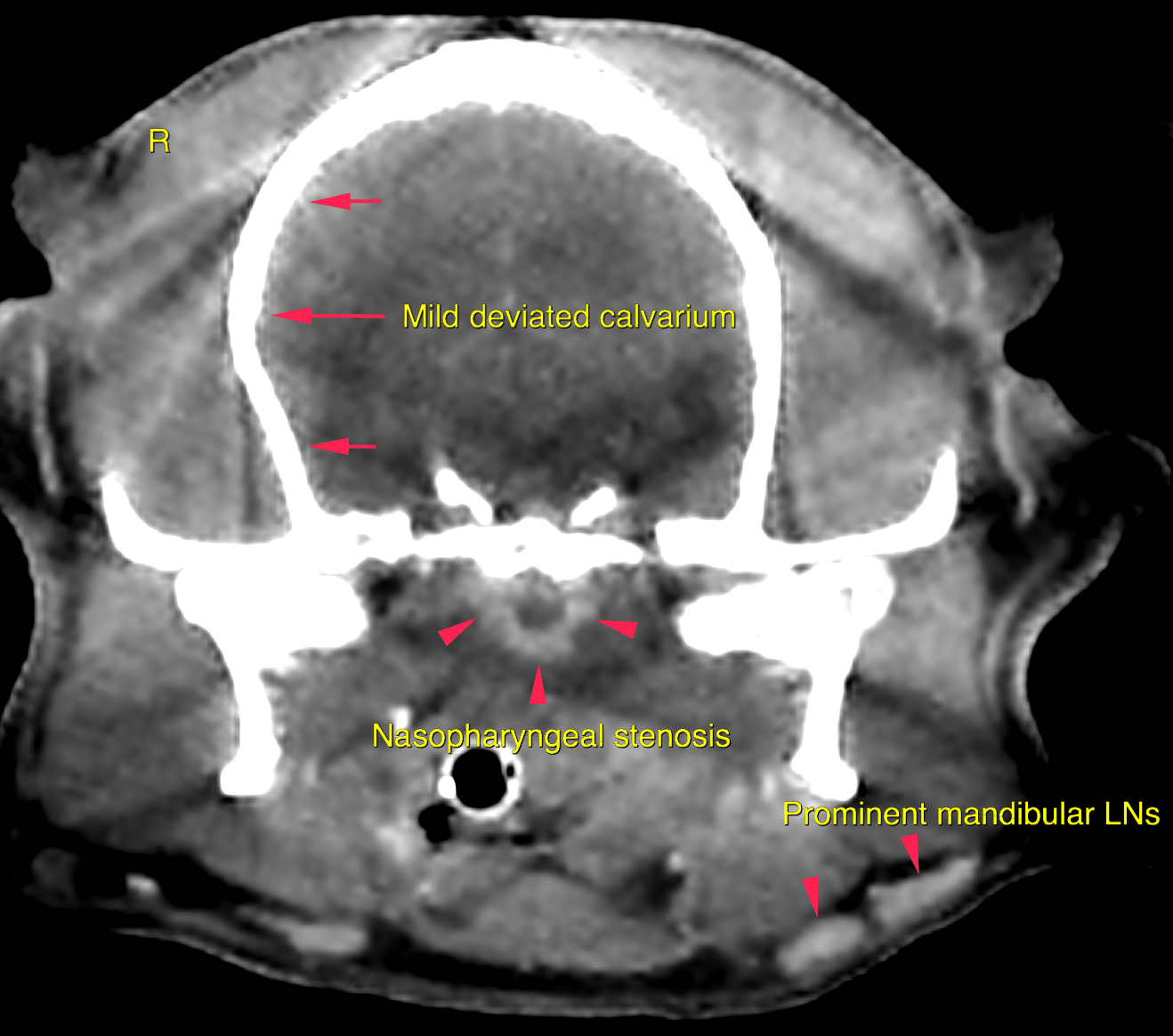
This 8 year old FS Brussels Griffon presented woitj bilateral, chronic nasal discharge that was non-responsive to antibiotics.
PE- overwieght, dermatitis, loud harsh cough during endotracheal intubation and upon recovery.
CBC/Chem – CK 243, Conj bilirubin 0.2, chol 379, Cl 105. UA – ammonium phosphate crystals +2
This 8 year old FS Brussels Griffon presented woitj bilateral, chronic nasal discharge that was non-responsive to antibiotics.
PE- overwieght, dermatitis, loud harsh cough during endotracheal intubation and upon recovery.
CBC/Chem – CK 243, Conj bilirubin 0.2, chol 379, Cl 105. UA – ammonium phosphate crystals +2