An 8-year-old NM DSH with a history of chemotherapy for metastatic mast cell neoplasia was presented for evaluation of tenesmus. On survey radiographs gas within the colon and lumbosacral degenerative disease was present.
An 8-year-old NM DSH with a history of chemotherapy for metastatic mast cell neoplasia was presented for evaluation of tenesmus. On survey radiographs gas within the colon and lumbosacral degenerative disease was present.
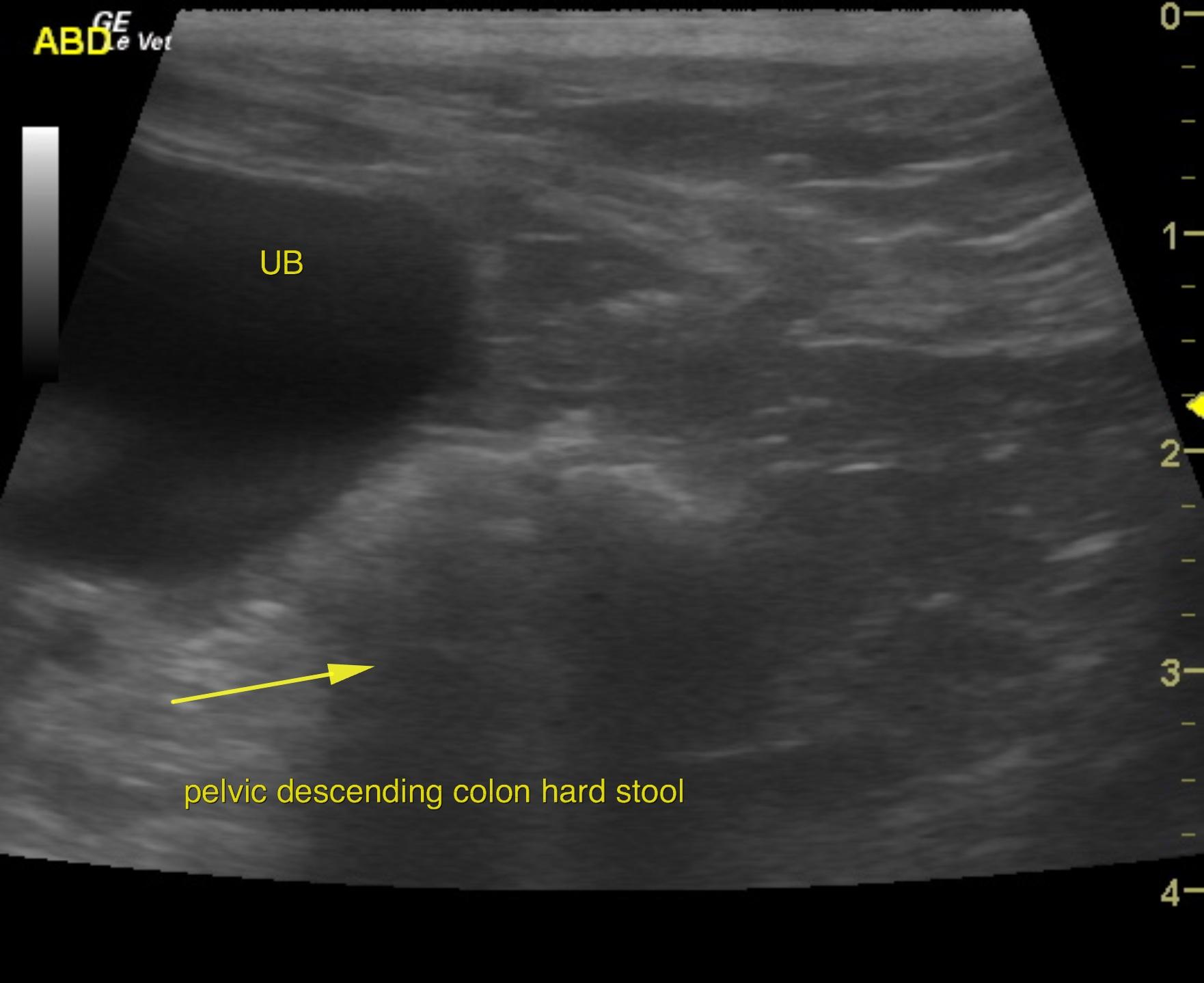
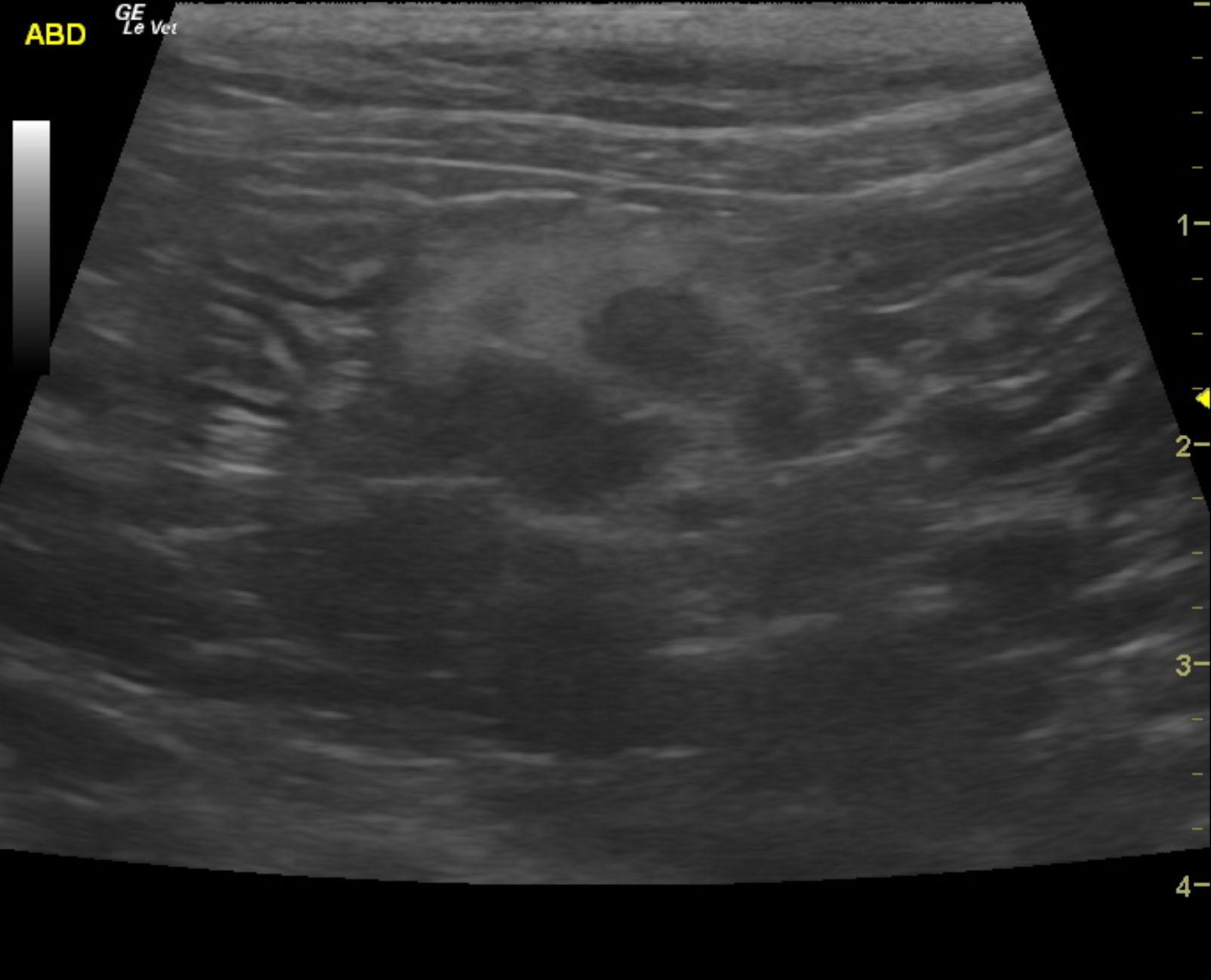
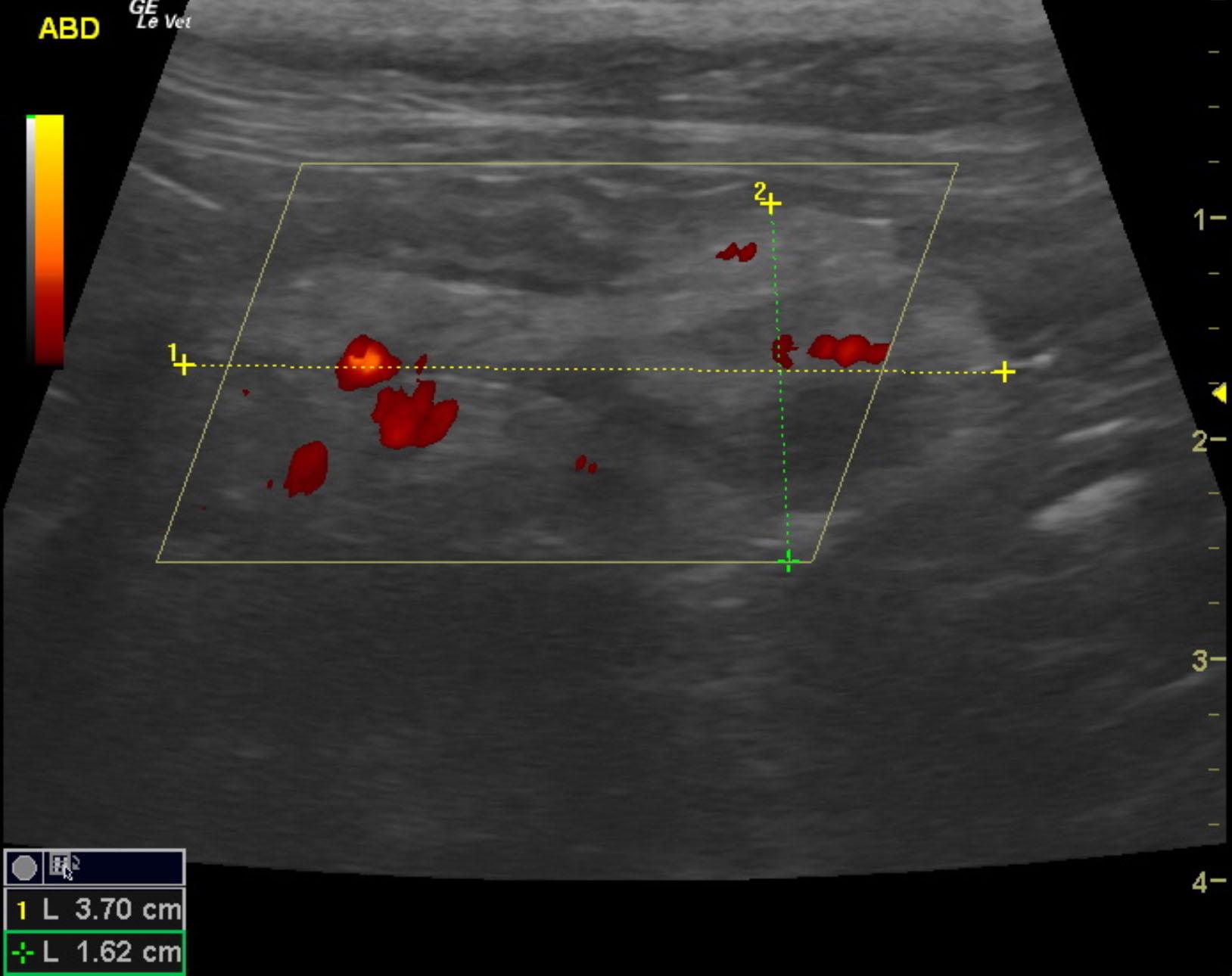
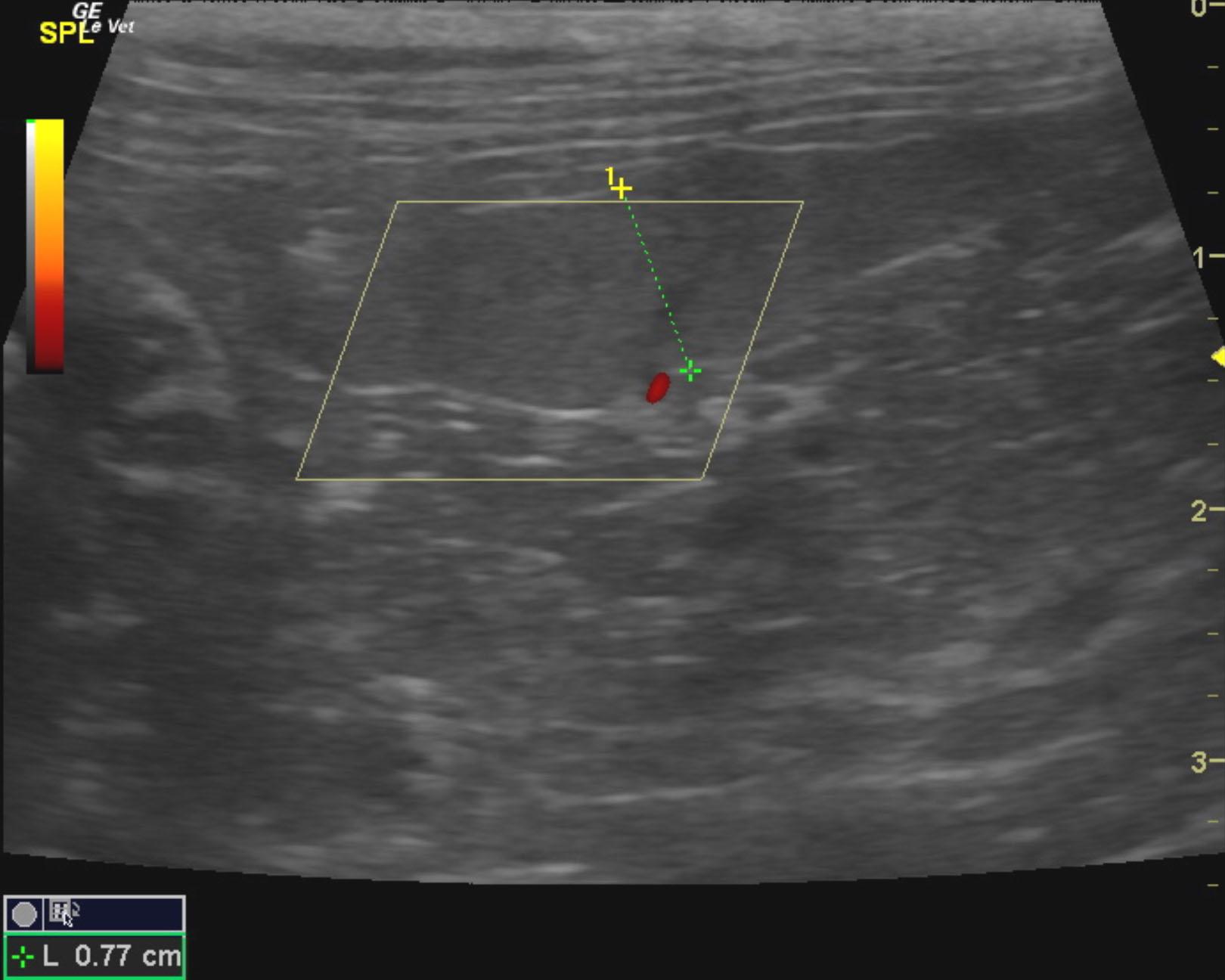
The visceral presentation sonographically revealed mesenteric lymphadenopathy with regional inflammation and adhesions, which is considered a partial remission. The small intestine is most consistent with inflammatory bowel type presentation. However, mast cell infiltration is also possible. The colonic wall appeared normal to the level of the pelvic inlet and where the hard stool is present on radiographs. The remainder of the colonic wall was unremarkable. Minor, irregular splenic contour with micronodular changes. Likely owing to infiltrative disease.
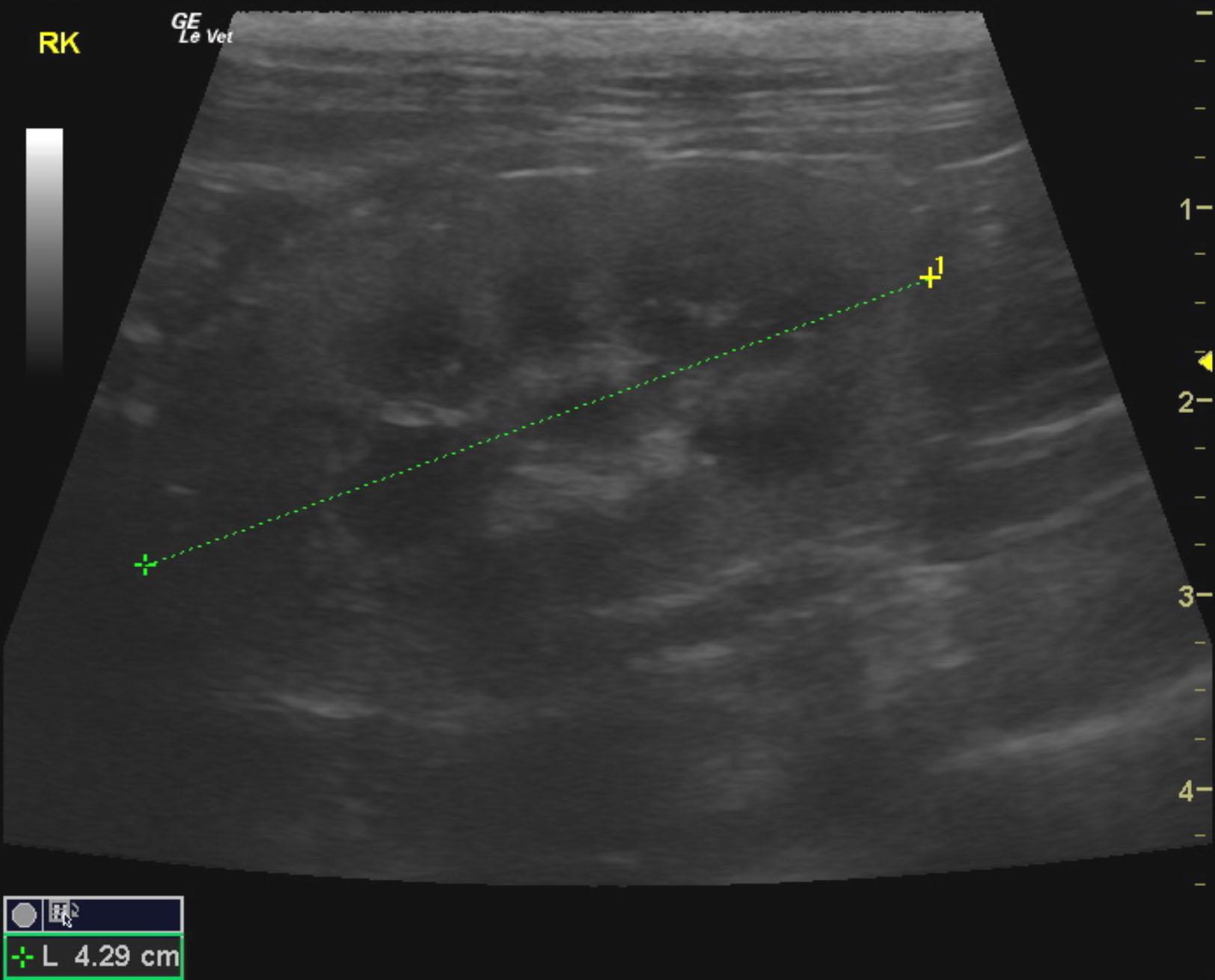
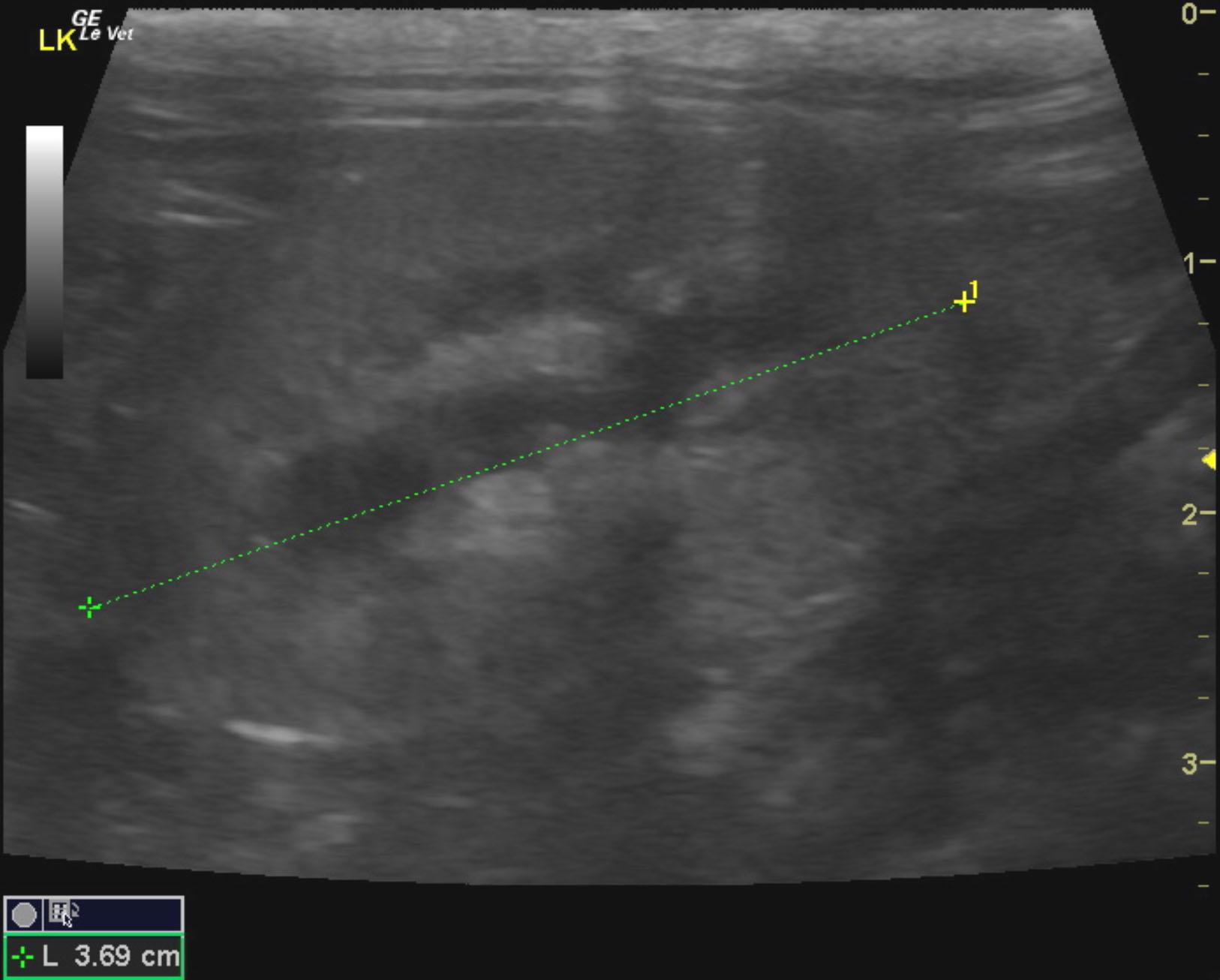
Degenerative renal changes with infarcts.
Variable small intestinal thickening was noted. The small intestine was empty as was the proximal colon. The descending colon revealed relatively hard stool at the level of the cystourethral junction. However, this should be resolvable with enema. No mural changes were noted in the visible colon, which was imaged to the level of approximately 3-4 cm past the cystourethral junction into the pelvic inlet. The mesenteric lymph nodes were enlarged and irregular measuring 2.0 x 1.0 cm with loss of detail and disrupted length to width ratio. Periserosal inflammatory pattern was noted. The cluster of lymph nodes measured approximately 3.7 x 1.6 cm including the mesenteric inflammation.
None
Colon – colitis, stenosis, obstipation, mega-colon
Pelvic canal – lymphadenomegaly, neoplasia, abscess, granuloma
Spine – disc disease, arthrosis, neoplasia
None