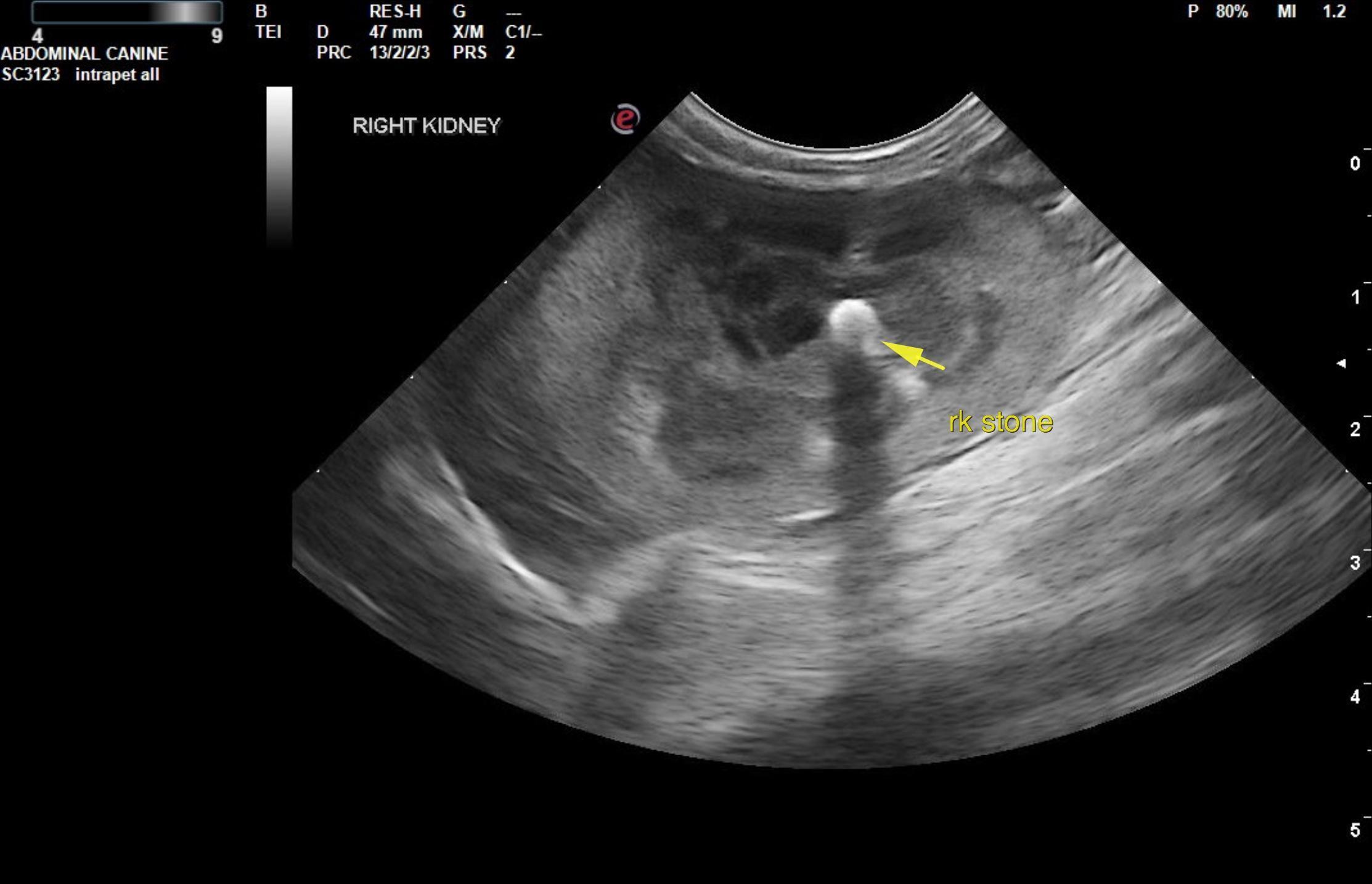
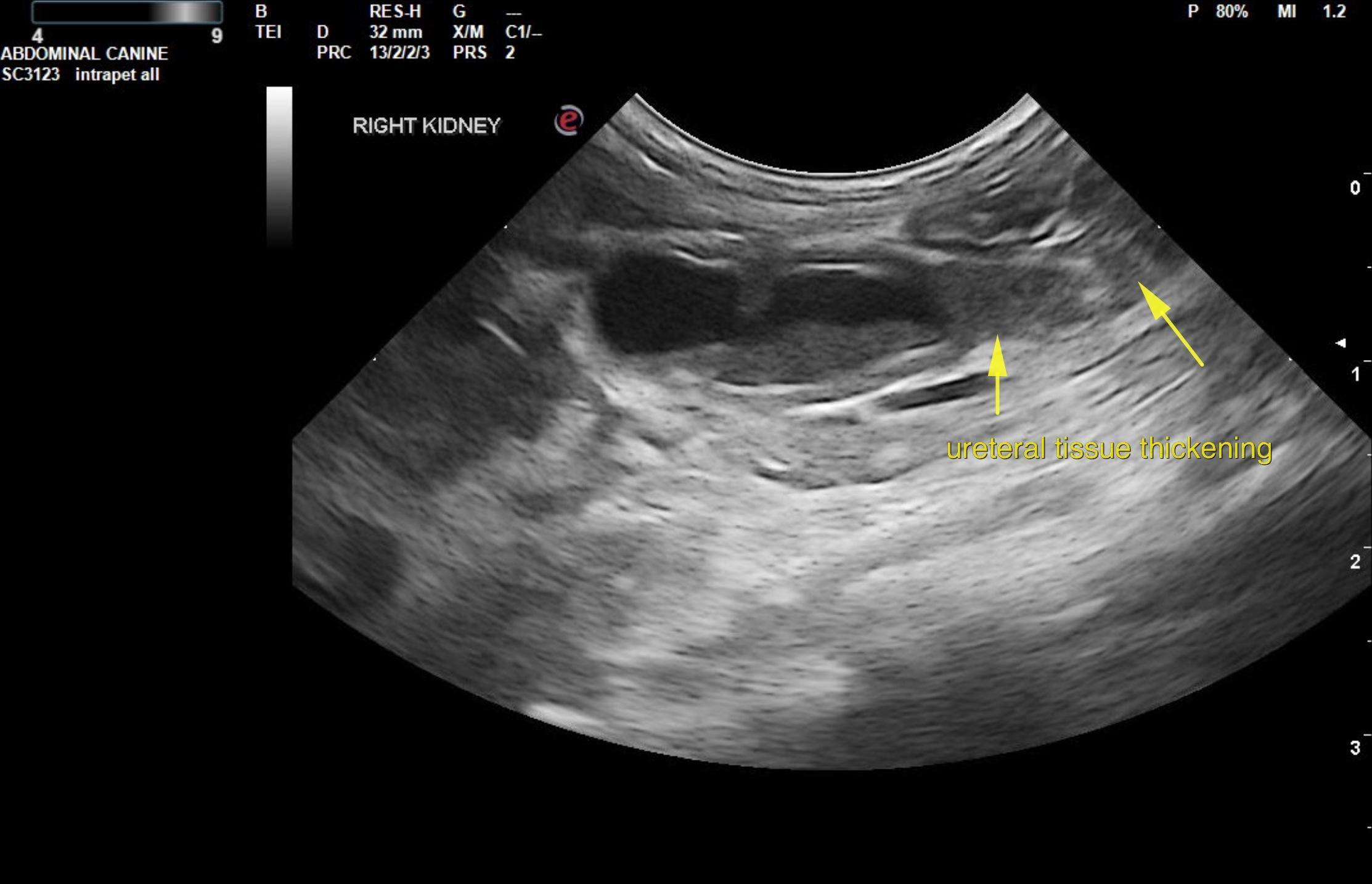
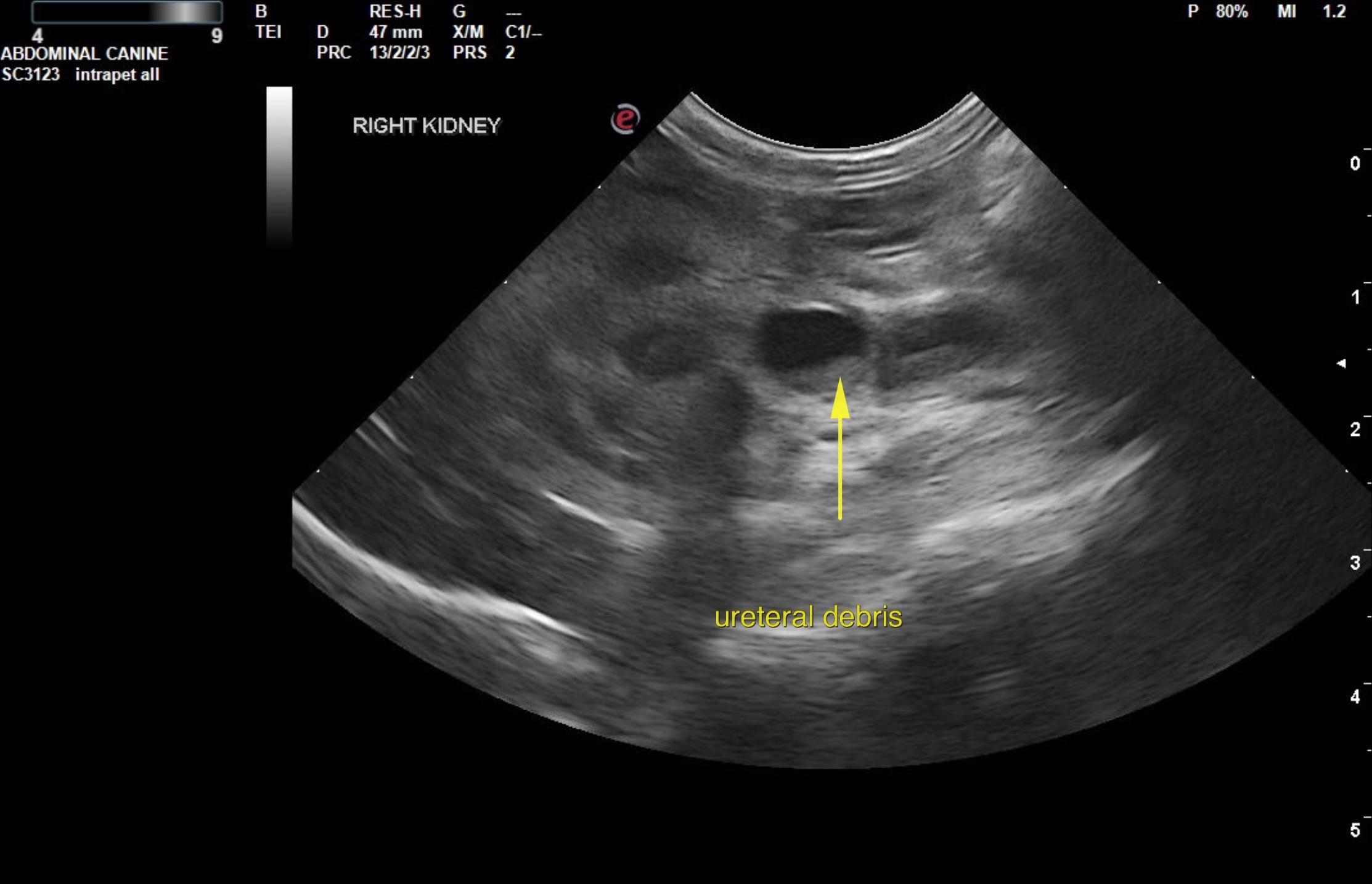
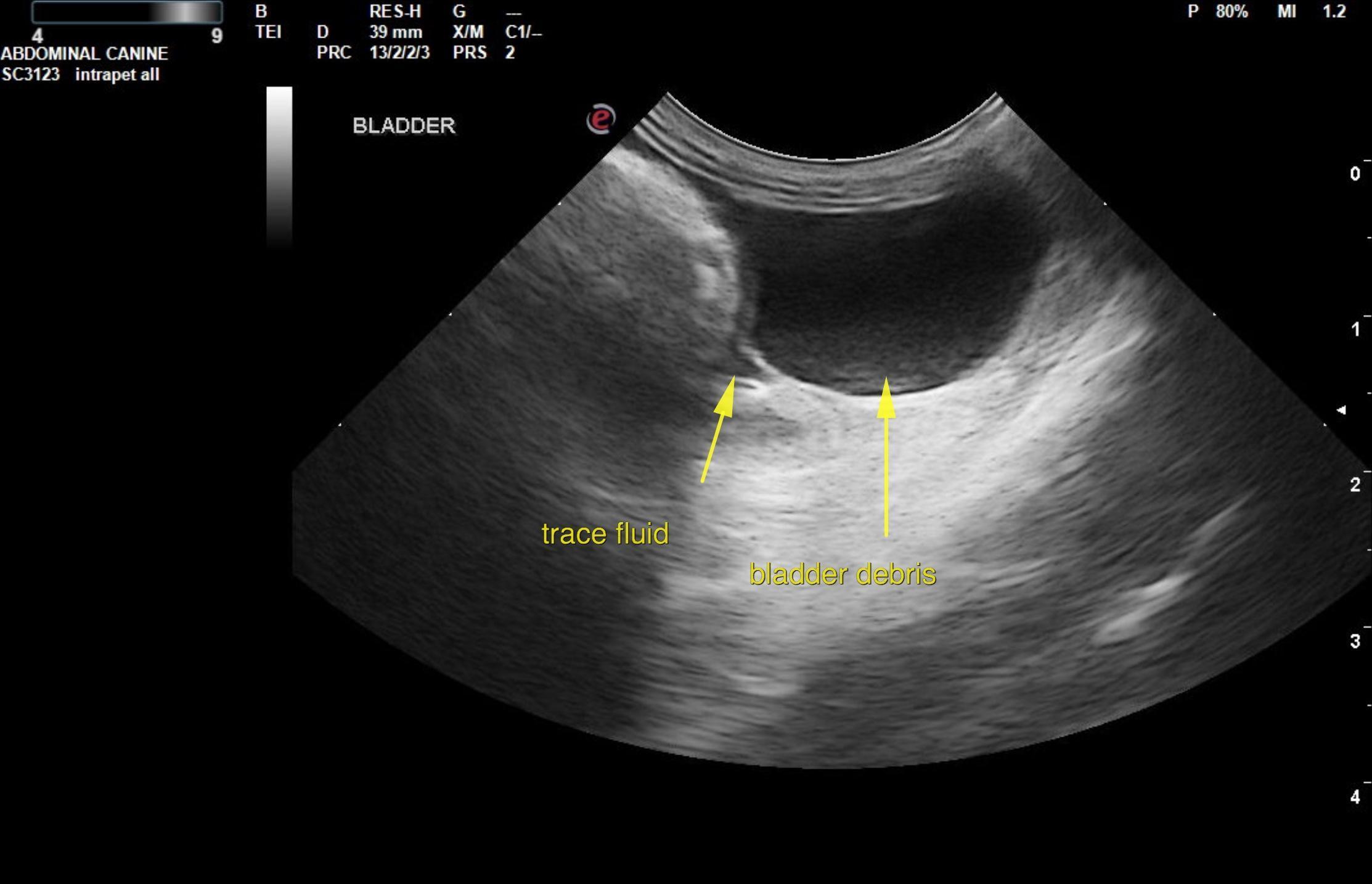
This 8 year old, 4 lbs, 11 oz DSH cat presented for weight loss, lethargic, no vomiting or diarrhea, unsure of eating, family moved homes ~ 1 week ago. PE: Temp 103 two days ago, 104.7 yesterday and 102 today. Total protein 9.2. Radiograph Findings: Opacities in area of kidneys poor detail due to decreased body fat.
This 8 year old, 4 lbs, 11 oz DSH cat presented for weight loss, lethargic, no vomiting or diarrhea, unsure of eating, family moved homes ~ 1 week ago. PE: Temp 103 two days ago, 104.7 yesterday and 102 today. Total protein 9.2. Radiograph Findings: Opacities in area of kidneys poor detail due to decreased body fat.