A 12-year-old FS Dachshund dog was presented at an emergency facility for intermittent vomiting and diarrhea lasting several weeks. The only obvious abnormality on physical examination was lethargy. She was treated with Famotadine, metronidazole, and discharged with a bland diet. At follow-up examination the following day at the RDVM, the owner reported that the patient had vomited twice and was having uncontrollable diarrhea. CBC and blood chemistry showed neutrophilia, lymphocytopenia, eosinopenia, elevated ALP activity, elevated CK, hyperamylasemia, and low TCO2. SPEC cPL was 173.
A 12-year-old FS Dachshund dog was presented at an emergency facility for intermittent vomiting and diarrhea lasting several weeks. The only obvious abnormality on physical examination was lethargy. She was treated with Famotadine, metronidazole, and discharged with a bland diet. At follow-up examination the following day at the RDVM, the owner reported that the patient had vomited twice and was having uncontrollable diarrhea. CBC and blood chemistry showed neutrophilia, lymphocytopenia, eosinopenia, elevated ALP activity, elevated CK, hyperamylasemia, and low TCO2. SPEC cPL was 173. Abdominal radiographs showed some loss of density in the cranial abdomen. The patient was treated with IV fluids, metronidazole, Ampicillin, and Cerenia.
Case Study
Typhlitis and lymphadenitis in a 12 year old FS Dachshund dog
Sonographic Differential Diagnosis
Perforating ileum at the ileocecal junction. Loss of detail, excessive wall thickness and lack of peristalsis combine to meet neoplastic criteria such as intestinal lymphoma, mast cell disease, or carcinoma. Complicated inflammatory disease (IBD, bacterial based enteritis), bowel infarction, and/or spontaneous perforation should also be considered.
Image Interpretation
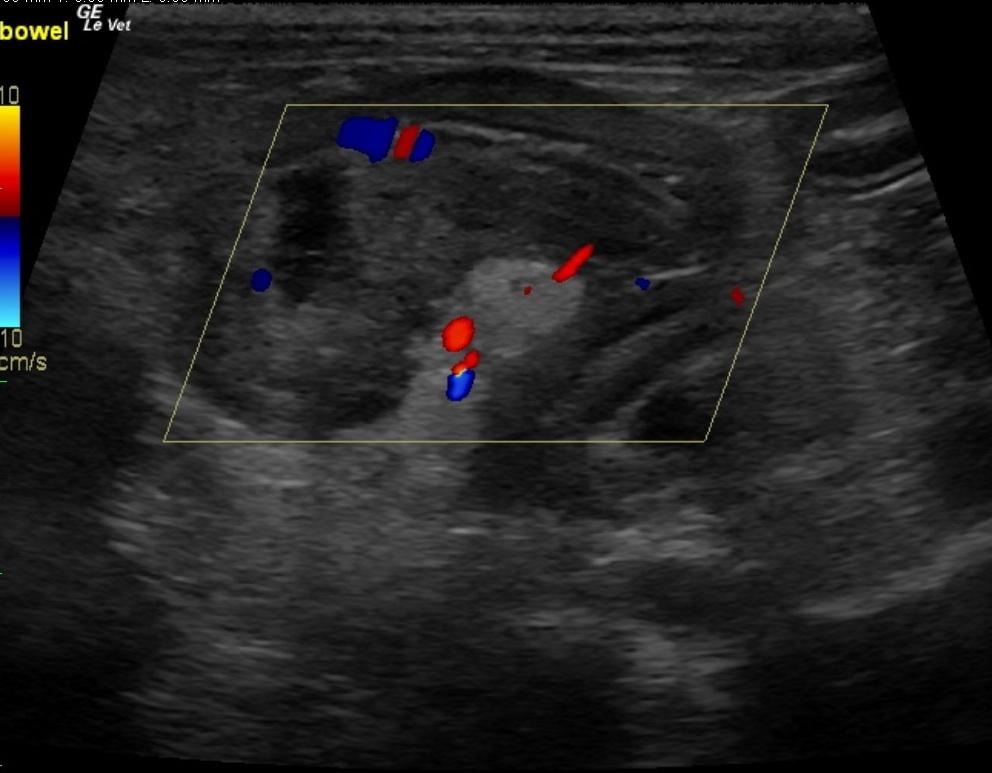
A long portion of distal ileum notes loss of mural detail within the intestinal wall along with periserosal echogenic fat associated with the bowel. This excessive wall thickness combined with loss of detail suggests transmural pathology, likely neoplastic in origin but potentially complicated inflammatory disease and emerging perforation may also be occurring. A high-resolution linear probe with virtual convex setting was used that enhances the detail of the hyperechoic omentum in the far field attached to the serosal layer and intestinal wall. This is the body’s own “Band-aid’ in order to wall off the pathology regardless of neoplastic or inflammatory in origin. Adhesions between the near field bowel and the far field bowel are present given the serpentine contour of the intestine linked together by the hyperechoic reactive and inflamed omentum…”natural omentopexy.” Color flow Doppler reveals positive signals in the region but lack of blood flow in the intestinal wall layer that lacks detail. Bowel infarction must be considered in this case. Video of the pathology shows the adhesion effect of the reactive omentum attached to the serosal layer of the bowel that lacks mural detail. The intestine gradually deviates away from a natural curvilinear infrastructure that is maintained in the far left of the screen and gradually and dramatically lost as one follows the intestine from left to right and into the adhesion. The patient demonstrated discomfort upon imaging of this region (+ Murphy Sign).
DX
Outcome
The patient had been recommended for immediate exploratory surgery with a plasma transfusion as well as assessment for pituitary dependent Cushing’s disease. Intra-operative ultrasound was also offered to determine further definition of healthy bowel. The patient underwent an exploratory laparotomy, which resulted in removal of the cecum, 2 inches of colon, and 2 inches of small intestine. Post-operative CBC only showed a low MCHC. Post surgery the patient developed multiple purulent skin lesions that lasted for approximately 2 weeks and did not resolve despite treatment with Simplicef or Amoxicillin. Biopsy of these lesions revealed chronic neutrophilic and lympho-histiocytic perivascular dermatitis ascribed to the intestinal lesions. Several weeks after surgery the owner reported that the patient was doing very well.
Comments
Title: December case of the month On Any Given Sunday: Meeting Sonographic Criteria For Intestinal Neoplasia But Neoplasia Doesn’t Win The Game. This is why we play the game, to ensure we don’t do “histopathological ultrasound” and not just call it neoplasia. Patient imaged by Andi Parkinson RDMS and medical management by Dr. Pam Nesbitt, Surgery By Dr. Joe Zulty, Essex Middle River Veterinary Center, Baltimore, MD, USA.
Clinical Differential Diagnosis
GI tract pathology (IBD, neoplasia, infection -bacterial/protozoa/fungal, partial obstruction); Pancreatic pathology (pancreatitis, neoplasia); Peritonitis
Sampling
Full-thickness surgical biopsies of both the cecum and lymph node revealed pyogranulomatous mural typhlitis and lymphadenitis, respectively.
Video
Patient Information
Clinical Signs
- Diarrhea
- Lethargy
- Vomiting
Exam Finding
- Lethargy
Images


Blood Chemistry
- Alkaline Phosphatase (SAP), High
- Amylase, High
- CPK, High
CBC
- Eosinophils, High
- Lymphocytes, High
- Lymphocytes, Low
- Neutrophils, High
Clinical Signs
- Diarrhea
- Lethargy
- Vomiting
Special Testing
- cPLI Negative