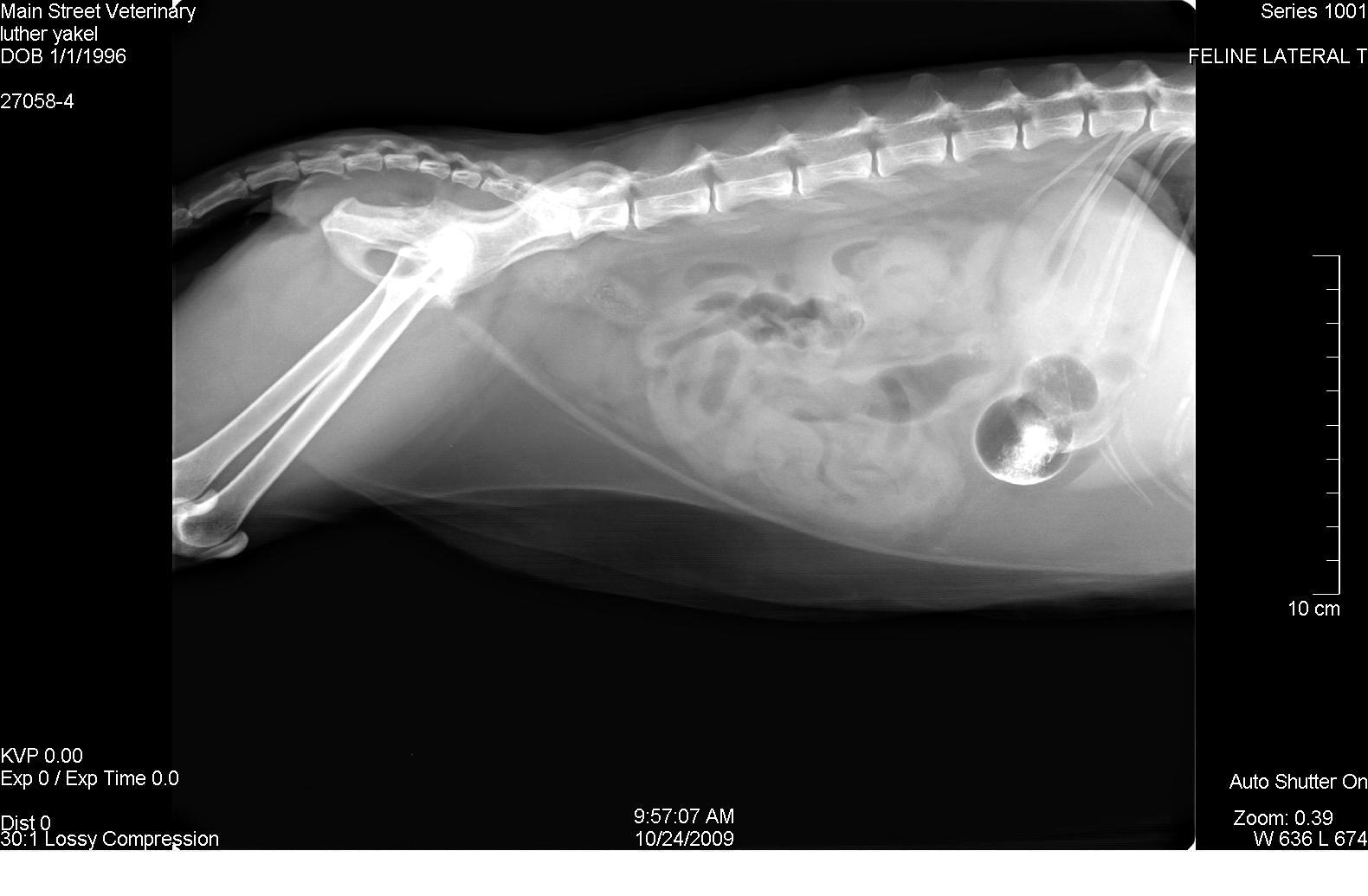
A 14-year-old MN DLH cat presented for anorexia, lethargy, and “not doing right”. The physical exam revealed depression, dehydration, and hypothermia. CBC revealed an elevated WBC count of 24,000 with a left shift and lymphocytopenia. Blood chemistry analysis was normal. Urinalysis revealed isosthenuria with neutral pH and negative culture. Radiographic Interpretation: (Images 1-3) The initial study shows a positive contrast distended stomach with evidence of segmental small bowel fluid and gas distention and adequate abdominal visceral serosal detail.
A 14-year-old MN DLH cat presented for anorexia, lethargy, and “not doing right”. The physical exam revealed depression, dehydration, and hypothermia. CBC revealed an elevated WBC count of 24,000 with a left shift and lymphocytopenia. Blood chemistry analysis was normal. Urinalysis revealed isosthenuria with neutral pH and negative culture. Radiographic Interpretation: (Images 1-3) The initial study shows a positive contrast distended stomach with evidence of segmental small bowel fluid and gas distention and adequate abdominal visceral serosal detail. The follow-up study reveals persistent gas and fluid distention of the stomach with retention of a small amount of contrast material. The degree and extent of small bowel fluid and gas distention has increased. The final study reveals generalized fluid and gas distention of the small intestine supportive of significant paralytic ileus or possibly mechanical ileus associated with a transient partially or intermittent foreign body within the distal small intestines.
Case Study
Transmural enteritis and peritonitis in a 14-year-old MN Domestic Long Hair cat
Sonographic Differential Diagnosis
Proximal enteritis with associated gastrointestinal paralytic ileus and peri-intestinal inflammation; Infiltration with lymphoma or an equivalent neoplastic process.
Image Interpretation
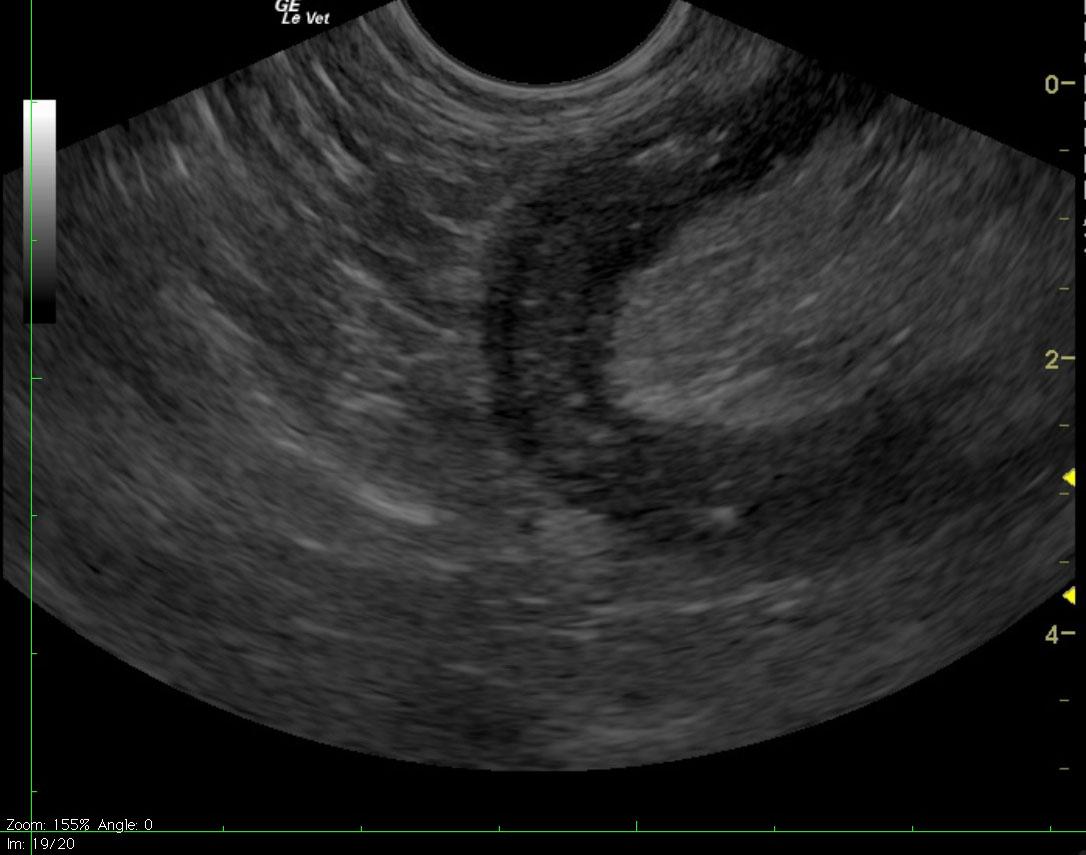
Ultrasound reveals marked gastric distention with fluid, dependent echogenic contents and a small amount of gas. Complete loss of gastric peristalsis appears to be present. Mild-to-moderate fluid distention of the proximal small intestines is also apparent. The proximal small bowel walls are thickened and hypoechoic with subtle loss of distinction between layers. The affected small intestines appear to be bordered by mildly echogenic mesenteric fat.
DX
Outcome
Laparotomy revealed diffuse necrotic bowel and multifocal peritonitis.The patient survived partial enterectomy and postoperative period but unfortunately died shortly afterward.
Comments
Thank you to Eddie Molesworth DVM and staff at Main Street Veterinary Hospital, Baltimore, MD, USA for presenting this interesting case for interpretation.
Clinical Differential Diagnosis
Infectious (pyelonephritis,bartonella, other); GI pathology (neoplasia); lymphosarcoma (LSA); renal insufficiency
Sampling
Full-thickness surgical biopsies. Histopathology revealed chronic severe transmural ulcerative and granulomatous enteritis with predominance of lymphocytic & plasmacytic infiltrates. No evidence of neoplasia.
Video
Patient Information
Clinical Signs
- "Not Doing Right"
- Anorexia
- Lethargy
Exam Finding
- Dehydration
- Depression
- Hypothermia
Images



CBC
- Left Shift
- Lymphocytes, Low
- WBC, High
Clinical Signs
- "Not Doing Right"
- Anorexia
- Lethargy
Urinalysi
- Isosthenuria Present