Presenting clinical signs: dyspnea and coughing. PE: no audible murmurs, muffled lung sounds.
Presenting clinical signs: dyspnea and coughing. PE: no audible murmurs, muffled lung sounds.
Presenting clinical signs: dyspnea and coughing. PE: no audible murmurs, muffled lung sounds.
Presenting clinical signs: dyspnea and coughing. PE: no audible murmurs, muffled lung sounds.
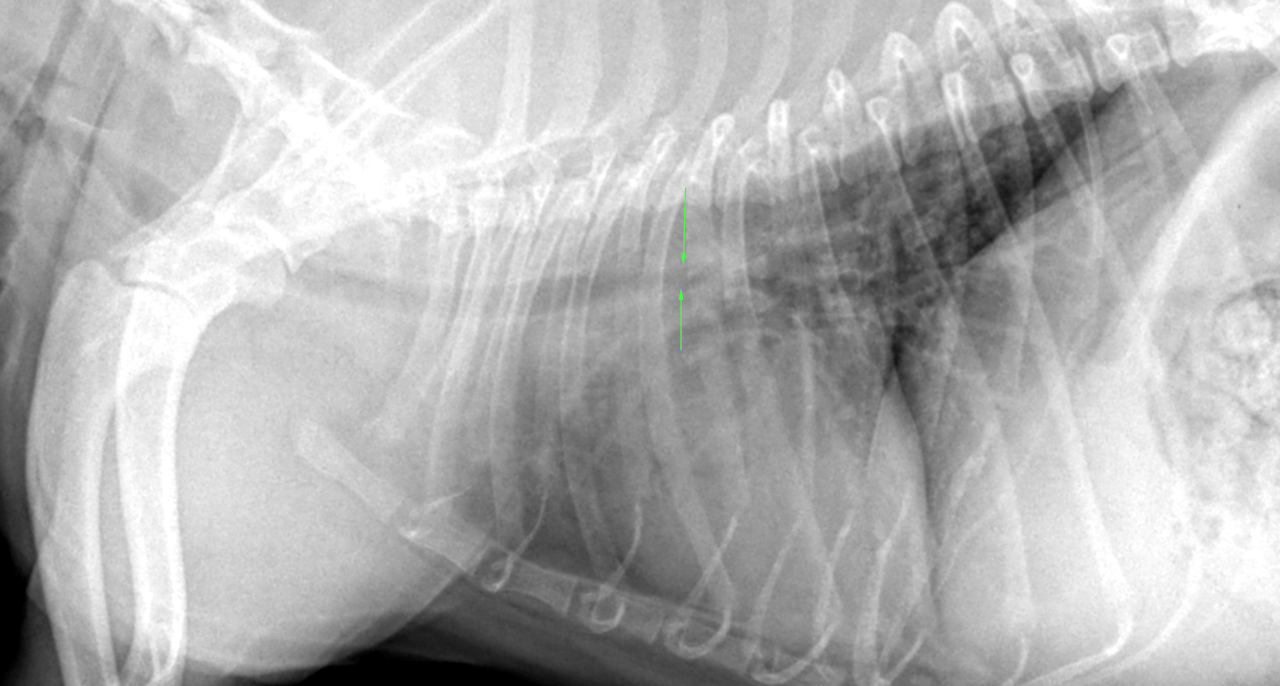
right lateral, left lateral and VD thorax- Osseous structures: There were mid thoracic wedge shaped hemivertebrae (T5 & T7)
Extrathoracic/-abdominal soft tissues: The patient was obese
Abdominal Structures:
The serosal detail was normal.
The liver was within normal limits.
The stomach contained a moderate amount of food and gas. There was a non
obstructive geometrically shaped mineral opaque foreign body within the gastric
fundus.
Intrathoracic structures:
The esophagus was not visible. The course of the trachea was normal. The tracheal cartilages were mineralized. The
intrathoracic trachea presented a prebirurcational dorsoventral flattening. The
bronchial tree was mineralized. There was a moderate generalized bronchial pattern
with peribronchial cuffing..
There was no mediastinal widening and no evidence of mediastinal lymph node
enlargement. There was no mediastinal shift.
The cardiac silhouette was within normal limits. The major and pulmonary vessels
were thin.
The radiographs do not identify evidence of cardiac pathology. There was aerophagia which likely was related to respiratory distress. For further diagnostic workup consider tracheobronchoscopy with bronchoalveolar lavage and rule out lung worms. The tracheal collapse is in a suboptimal position for stenting and multifocal or general bronchomalacia is likely to be present although not radiographically seen (most cases go undetected on radiographs). So, interventional treatment options are limited and symptomatic treatment and supportive care seems to be the appropriate measures here although not ideal.
Weight management may also be helpful to alleviate the clinical signs