A 1-year-old F Dachshund dog was presented for lethargy, anorexia, difficulty breathing, and unusual behavior. The only abnormality on CBC and serum chemistry was hypoproteinemia. Radiographs revealed pleural and abdominal effusion. The pleural effusion was quantified as a transudate containing predominantly lymphocytes. Urinalysis and bile acids were both within normal limits.
A 1-year-old F Dachshund dog was presented for lethargy, anorexia, difficulty breathing, and unusual behavior. The only abnormality on CBC and serum chemistry was hypoproteinemia. Radiographs revealed pleural and abdominal effusion. The pleural effusion was quantified as a transudate containing predominantly lymphocytes. Urinalysis and bile acids were both within normal limits.
Case Study
Protein Losing Gastritis/Enteritis (PLE) in a 1 year old F Dachshund dog
Sonographic Differential Diagnosis
PLE due to underlying IBD, lymphangiectasia, neoplastic infiltrative change.
Image Interpretation
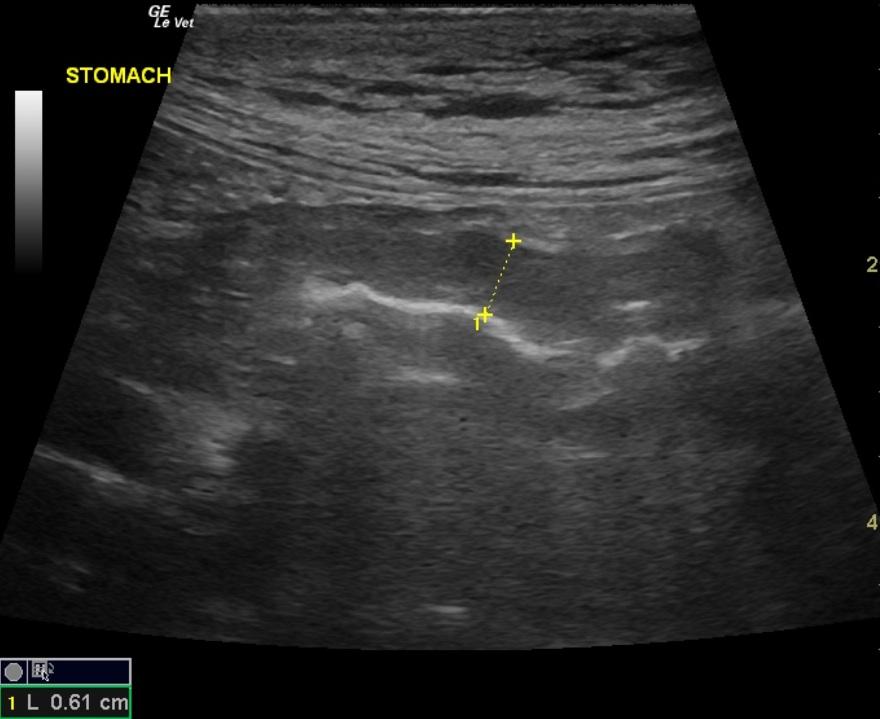
Thickened gastric mucosal layer with hypoechoic appearance. Subcutaneous edema is noted.Marked pleural effusion cranial to diaphragmatic interface, no evidence of CVC dilation, trace effusion noted in periportal region cranial to stomach. Pyloric wall is mildly thickened. High resolution of the small intestinal wall reveals mucosal stippling or striations which would suggest inflammation and lymphangectasia respectively. COMMENT: Due to intermittent machine difficulties, in this case, there is an echopoor band in the near field of all images made with the curvilinear transducer. The sonographer, having experience with this anomaly, was able to evaluate the tissues and correct for this problem with the use of the high frequency linear transducer, see Image 1. Video 3: Ascites. Notice near field small intestinal segment has loss of wall architectural detail and there is a hyperechoic irregular serosal surface. Compare to small intestinal segment in far field with more normal appearance, visible layering, and lack of serosal irregularity.
DX
Comments
The ascites and pleural effusion in this case was owing to loss of oncotic pressure from albumin loss. As a rule, when the albumin level is less than 1.5 g/dl, third spacing of fluid (ascites, pleural effusion) may occur spontaneously. If the albumin is subnormal, but higher than 1.5 g/dl, then the clinical sonographer should look for concurrent pathology such as lymphatic obstruction, portal hypertension to justify a physical obstruction contributing to the ascites formation.
The dog was treated with metronidazole, prednisone and fed Hills r/d diet. A week later azathioprine was added. A month later the dog was on azathioprine, prednisone, and the r/d diet.
Clinical Differential Diagnosis
hypoproteinemia – lymphangiectasia (congenital, secondary to neoplasia, IBD), IBD.
Sampling
Biopsies from the stomach and intestines showed mild lymphoplasmacytic gastritis and moderate lymphoplasmacytic enteritis.
Video
Patient Information
Clinical Signs
- "Not Doing Right"
- Anorexia
- Dyspnea
- Lethargy
Images
Blood Chemistry
- Total Protein, Low
Clinical Signs
- "Not Doing Right"
- Anorexia
- Dyspnea
- Lethargy