A 10-year-old MN Golden retriever was presented for lethargy and inappetence. No abnormalities were noted on the physical exam. The following day hematochezia was reported. CBC was within normal limits. Blood chemistry profile revealed elevated cholesterol , elevated total bilirubin, elevated direct bilirubin, hypoproteinemia, hypoalbuminemia, and hypocalcemia. Urinalysis revealed hematuria and bilirubinuria.
A 10-year-old MN Golden retriever was presented for lethargy and inappetence. No abnormalities were noted on the physical exam. The following day hematochezia was reported. CBC was within normal limits. Blood chemistry profile revealed elevated cholesterol , elevated total bilirubin, elevated direct bilirubin, hypoproteinemia, hypoalbuminemia, and hypocalcemia. Urinalysis revealed hematuria and bilirubinuria.
Case Study
Necrotizing enteritis with perforation in a 10 year old MN Golden Retriever dog
Sonographic Differential Diagnosis
Complicated inflammatory event or bowel infarction of the distal small intestine adjacent to the urinary bladder. Possible emerging neoplasia such as mast cell disease or lymphoma.
Image Interpretation
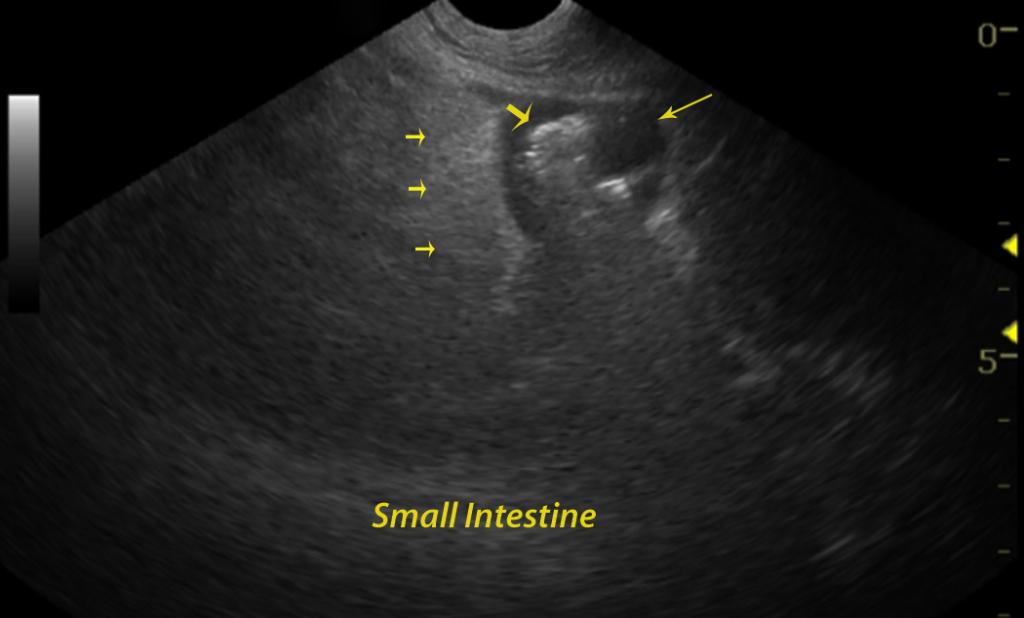
The gastrointestinal tract was largely normal in the upper gastrointestinal tract, however the mid small intestine and distal small intestine in the region of the urinary bladder presented diffuse thickening with mural detail loss. Adhesion pattern was noted associated with the small intestine. A separate portion of mid small intestine appeared also thickened with mild adhesion.
DX
Outcome
The patient was presented 5 days postoperatively for the evaluation of anorexia. Sonographic findings showed presence of an abdominal effusion and analysis of the abdominal fluid was consistent with peritonitis. An exploratory was declined by the owner. Full recovery was achieved by medical therapy alone and the patient was asymptomatic 3 months later.
Comments
Intestinal resection is essential.
Clinical Differential Diagnosis
GI pathology (Neoplasia – lymphoma, adenocarcinoma, mast cell tumor, leiomyoma, leiomyosarcoma; colitis due to inflammatory bowel disease, foreign body, abscess, granuloma); hepatic pathology (cholangiohepatitis, mucocele) ; chronic active pancreatitis; pyelonephritis; hypoadrenocorticism
Sampling
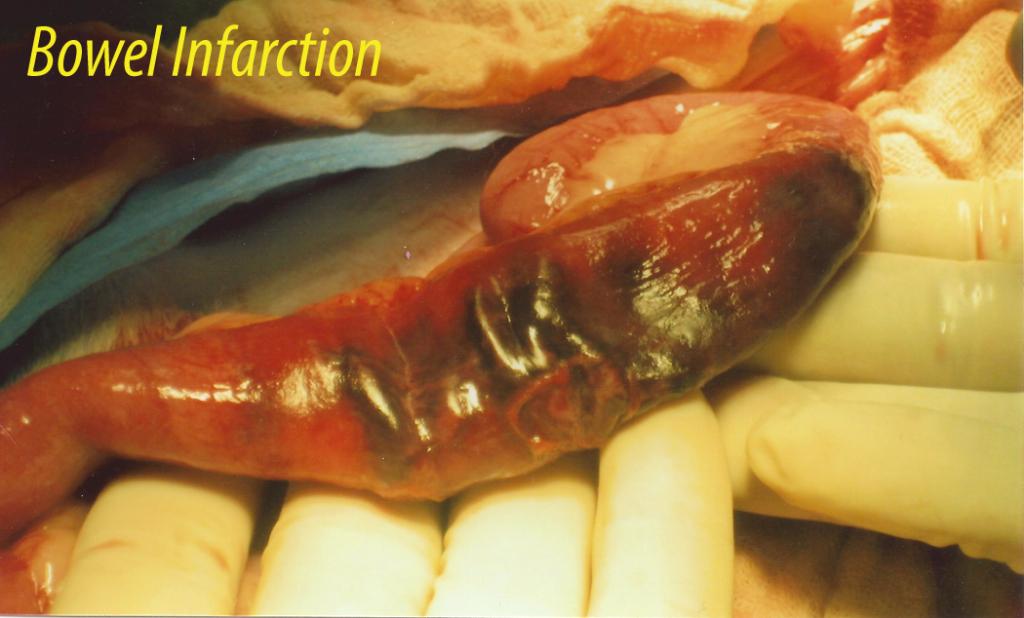
An exploratory laparotomy revealed a perforated small intestine. Ten inches of small intestine were resected with no foreign body present. Histopathology revealed severe sub acute necrotizing enteritis and multifocal enteric vasculitis and thrombosis. The culture of the intestinal wall showed growth of two bacteria: Escherichia coli 3+ and Enterococcus species 3+.
Video
Patient Information
Clinical Signs
- Anorexia
- Fresh Blood in Stool
- Lethargy
Images
Blood Chemistry
- Albumin, Low
- Calcium, Low
- Cholesterol, High
- Total Bilirubin, High
- Total Protein, Low
Clinical Signs
- Anorexia
- Fresh Blood in Stool
- Lethargy
Urinalysi
- Bilirubin Present
- Blood Present