History: Several months ago had an acute episode of form pitting edema that progressed to subcutaneous hemorrhage within 24 hours. Resolved within a few days. Treated with steroid injection. Tick serology was negative. Clotting panel normal except for elevated fibrinogen. Serumchemistry normal except for low creatinine. Yesterday developed acute swelling of left hind leg that progressed to subcutaneous hemorrhage today. She is experiencing tachypnea, tongue is pink.
Physical Exam: NSF except for tachypnea.
History: Several months ago had an acute episode of form pitting edema that progressed to subcutaneous hemorrhage within 24 hours. Resolved within a few days. Treated with steroid injection. Tick serology was negative. Clotting panel normal except for elevated fibrinogen. Serumchemistry normal except for low creatinine. Yesterday developed acute swelling of left hind leg that progressed to subcutaneous hemorrhage today. She is experiencing tachypnea, tongue is pink.
Physical Exam: NSF except for tachypnea.
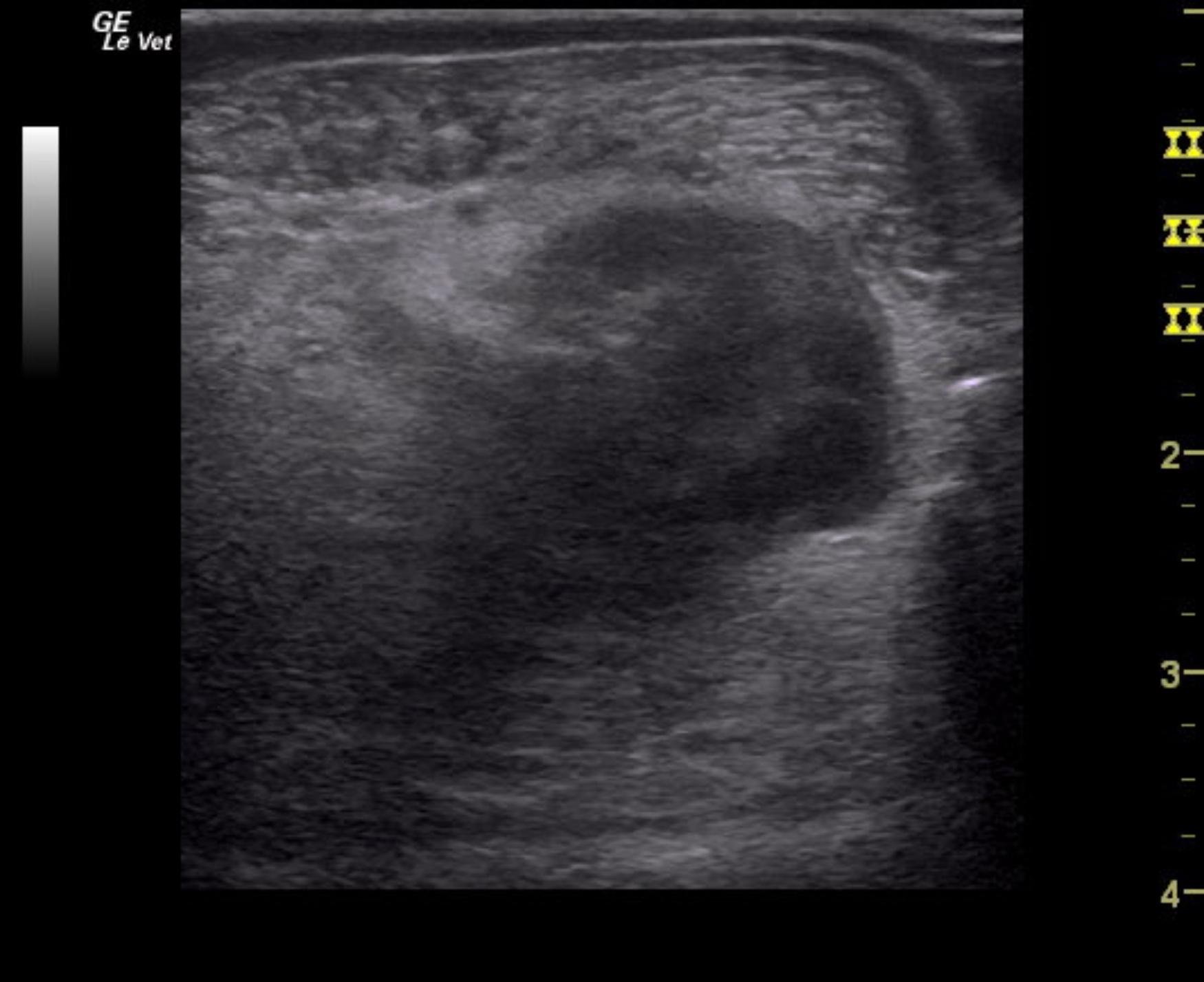
Reason for Ultrasound Exam: Very significant diffuse military lung pattern.