A 7-month-old NM DLH was presented for evaluation of an ejection murmur that had been detected at time of neuter.
A 7-month-old NM DLH was presented for evaluation of an ejection murmur that had been detected at time of neuter.
A 7-month-old NM DLH was presented for evaluation of an ejection murmur that had been detected at time of neuter.
A 7-month-old NM DLH was presented for evaluation of an ejection murmur that had been detected at time of neuter.
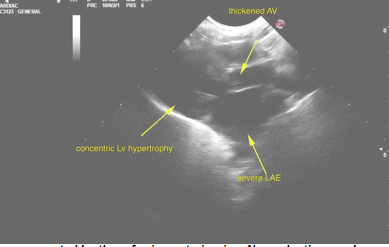
Hypertrophic Cardiomyopathy
Left sided congestive heart failure.
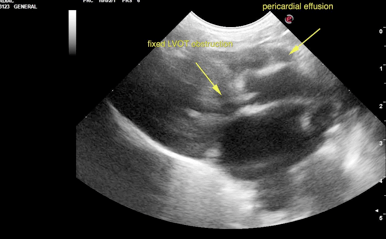
Slight pericardial effusion.
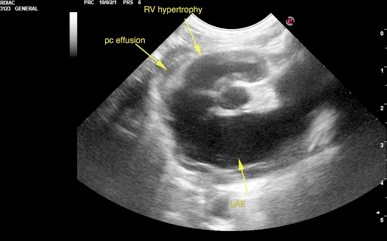
Right ventricular obstructive cardiomyopathy.
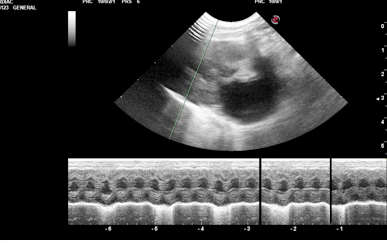
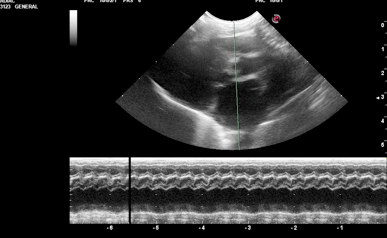
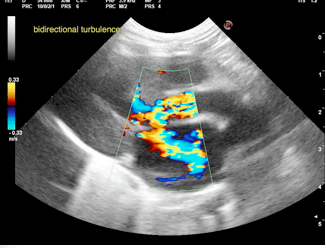
The cardiac presentation in this patient presented moderate to severe volume overload of the left atrium. The left atrium revealed concentric hypertrophy. The cranial and caudal mitral valve leaflets presented normal linear structure, extension in systole, and union in diastole. No significant dystrophic or vegetative changes were noted. The left ventricle revealed concentric hypertrophy. Hypocontractility was noted. The left ventricular outflow tract demonstrated dynamic and fixed obstruction. The aortic valve was thickened. This may be a secondary or primary congenital issue. The ventricular septum appeared to be intact. The right atrium was enlarged at 1.5 cm. Right ventricular hypertrophy was also noted. Tricuspid valvular assessment demonstrated adequate linear morphology. The pulmonary artery appeared dilated in this patient. A trace amount of pericardial effusion was noted. The cranial mediastinum and pericardial regions were free of masses in the visible window. Occasional arrhythmia was noted during the exam. LA max 2.5cm, LA/AO June Boon 2.5
Variable lung consolidations were noted.
No overt evidence of congenital defects were noted in this patient. However, further Doppler assessment of the right ventricular outflow and deep pulmonary artery would be warranted. However, regardless the prognosis is very poor long term. Recommend Lasix and ace inhibitor therapy at this point along with ECG to assess for arrhythmogenic activity. Plavix therapy would also be warranted. Recheck sonogram is recommended in 1-2 weeks. This patient is at risk for sudden death.
Atrial/ventricular septal defect, cardiomyopathy (hypertrophic, restrictive, dilated)