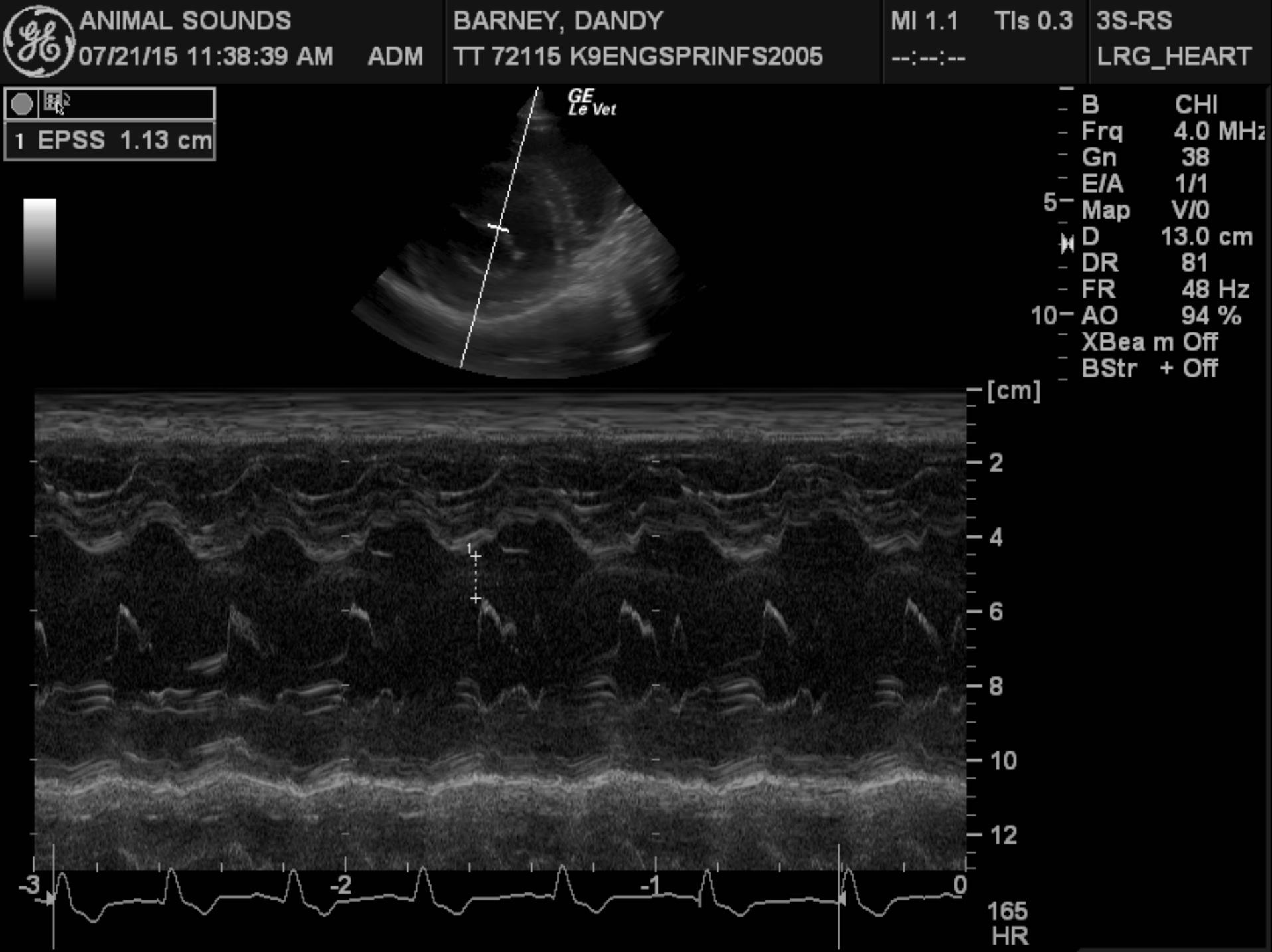
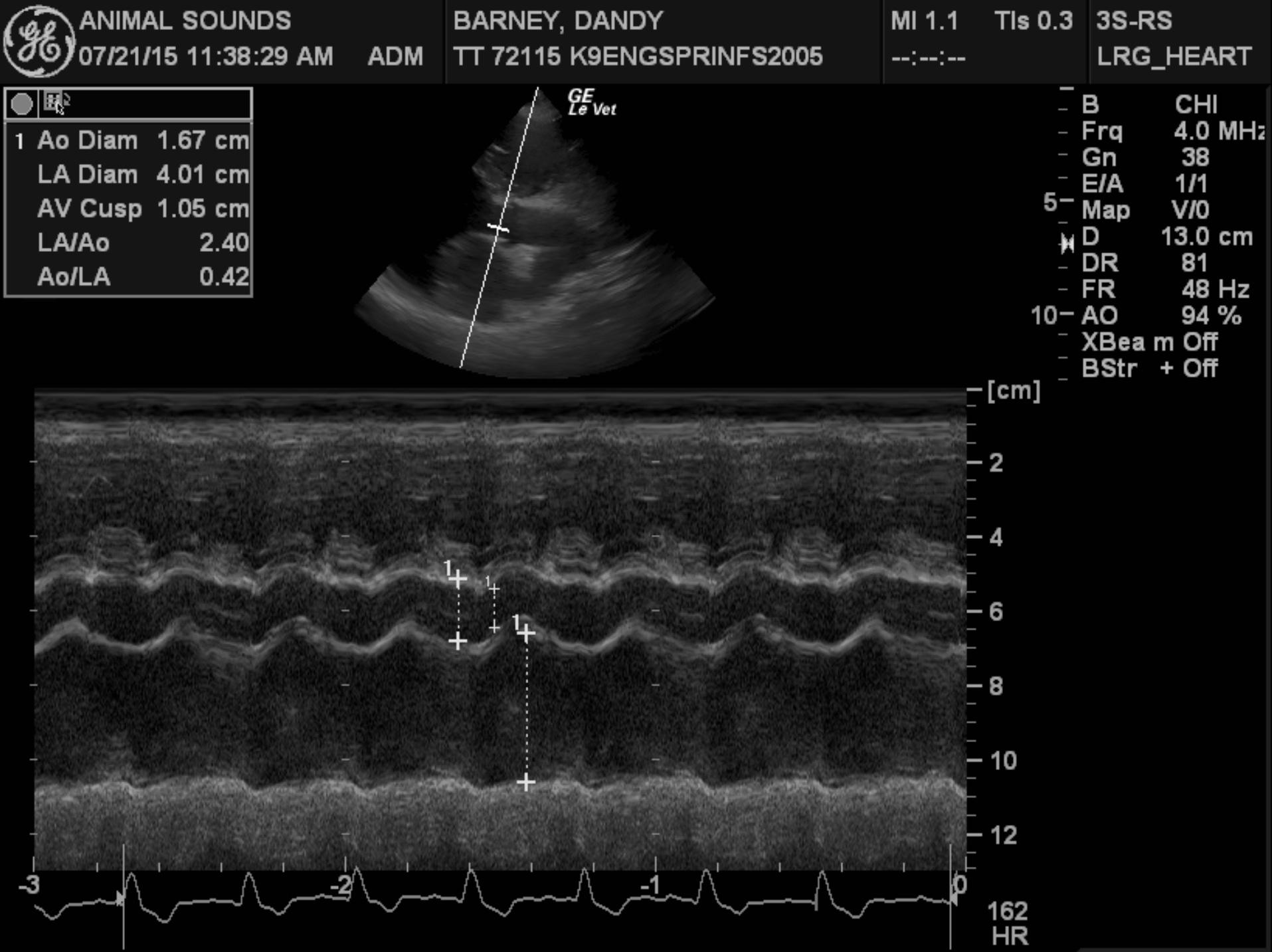
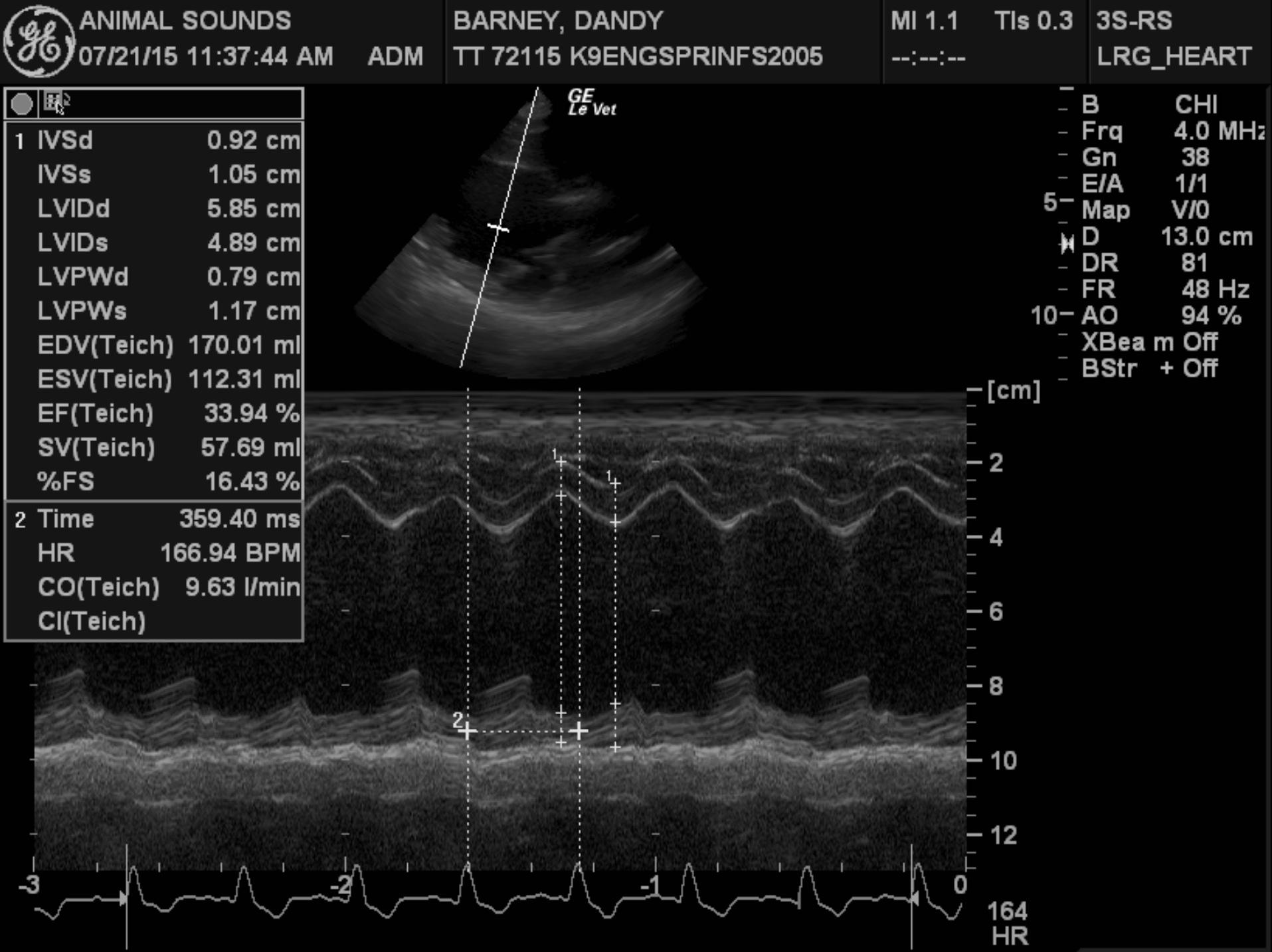
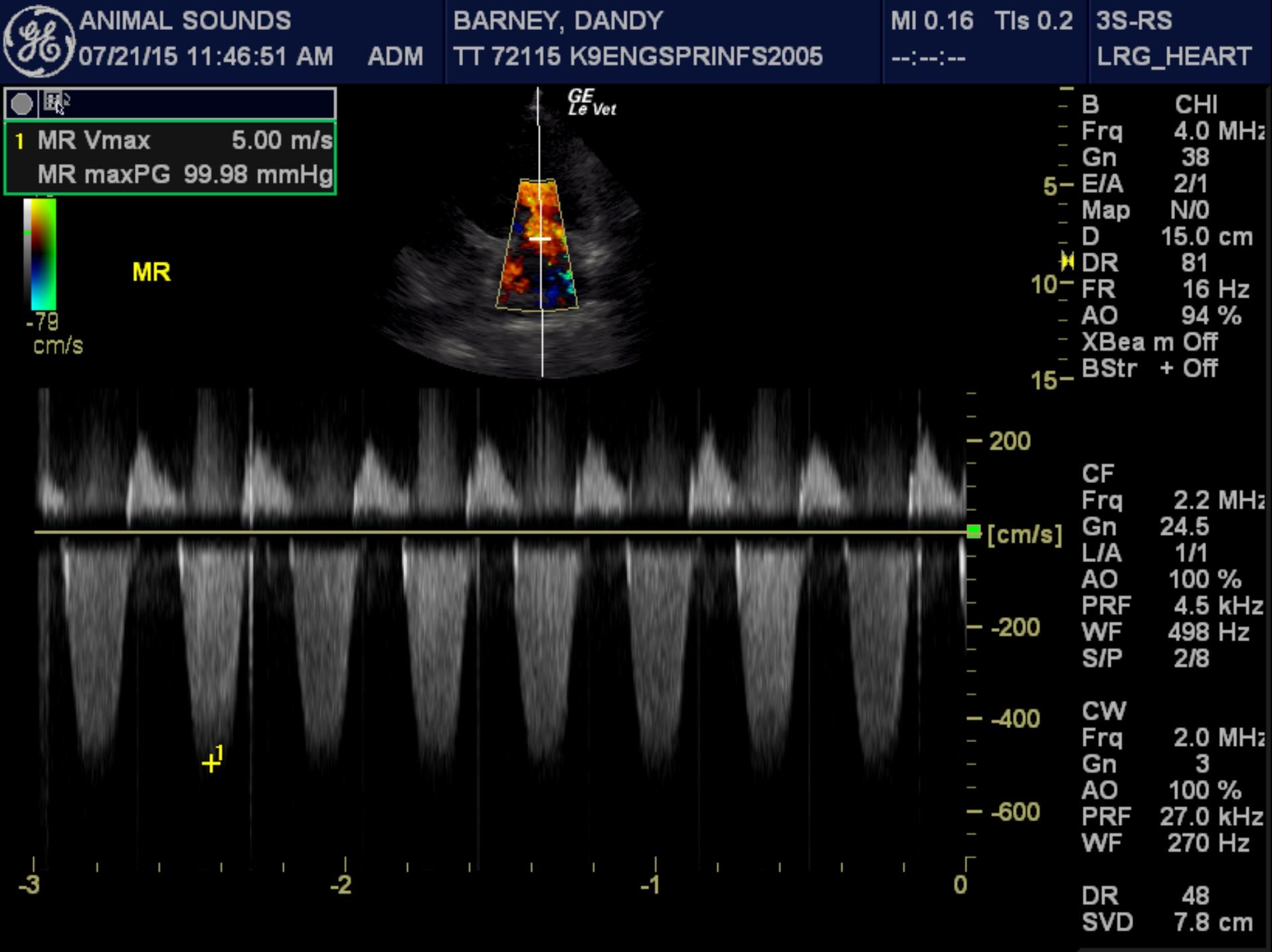
This examination demonstrates global left ventricular systolic dysfunction, consistent with dilated cardiomyopathy. Secondary to the patient’s myocardial dysfunction, she has severe left ventricular dilation, as well as moderate to severe left atrial dilation, and it appears that she is in mild congestive heart failure based on her thoracic radiographic findings. Given the severity of her cardiac disease, it appears very likely that this is the cause of her arrhythmia.
Unfortunately, the long-term prognosis for primary DCM is relatively poor, as the median survival following the first onset of congestive heart failure is in the 6-12 month range, though a small percentage of dogs do live significantly longer than this time period. The prognosis can be much better if a secondary cardiomyopathy, such as taurine deficiency or myocarditis, is present, as these diseases are potentially reversible, though they are much less common than primary DCM.
RECOMMENDATIONS: While taurine deficiency is unlikely, it is worthwhile to evaluate a plasma taurine level and to supplement with taurine (500 mg BID) pending the results.
Recommended therapy for the cardiac disease includes Lasix (50 mg BID), enalapril (10 mg BID), pimobendan (7.5 mg am, 5 mg pm), and spironolactone (25 mg BID).
Regarding the arrhythmia, while sotalol is effective against both APC’s and VPC’s, the negative inotropic properties of the medication can worsen the heart failure. Options would be to wait until the CHF is better controlled and then slowly introduce the sotalol, or alternatively, use different antiarrhythmics to treat the APCs and VPCs. A safer alternative to treat the ventricular ectopy would be mexiletine (100 mg TID with food, needs to be compounded). As for the atrial ectopy, therapy with diltiazem (15 mg TID) will likely be effective.
A recheck X-ray, renal profile, and ECG are recommended in one week.