This MN dog presented with nasal bleeding with congestion.
This MN dog presented with nasal bleeding with congestion.
This MN dog presented with nasal bleeding with congestion.
This MN dog presented with nasal bleeding with congestion.
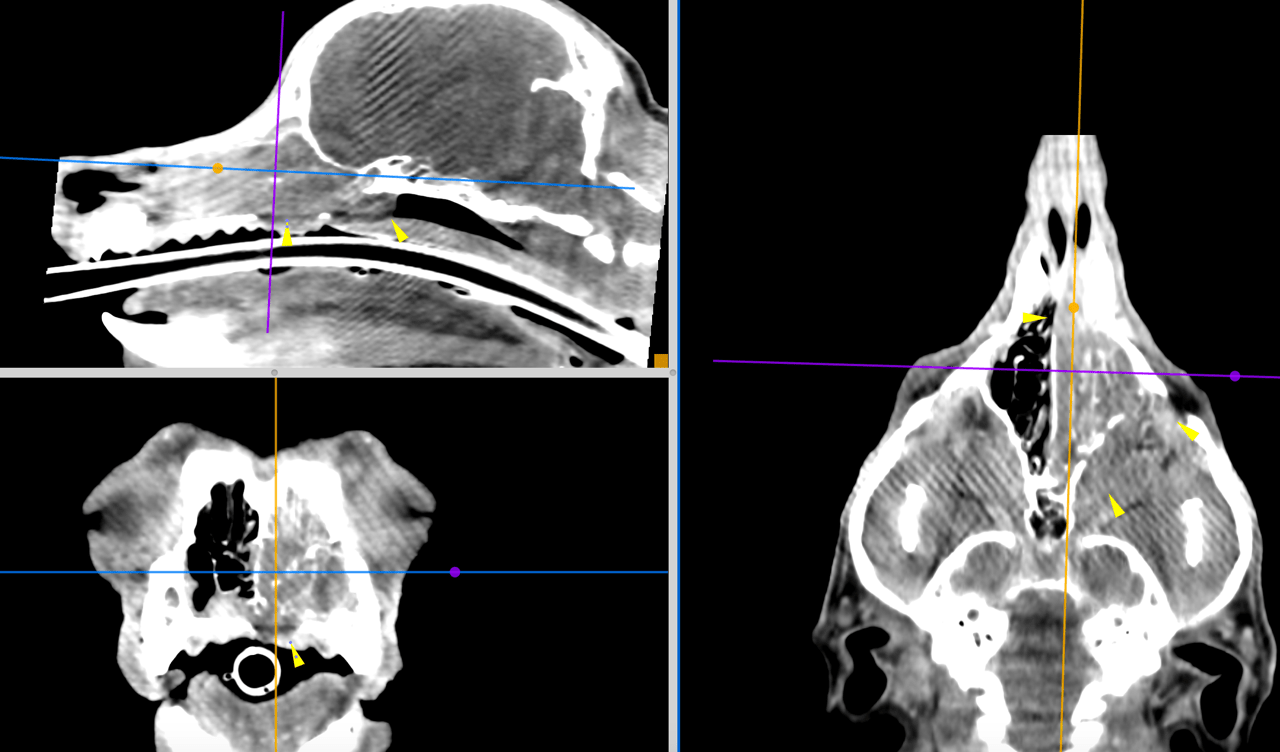
CT of the head, plan and post contrast – There is a large soft tissue attenuating space-occupying lesion within the left nasal
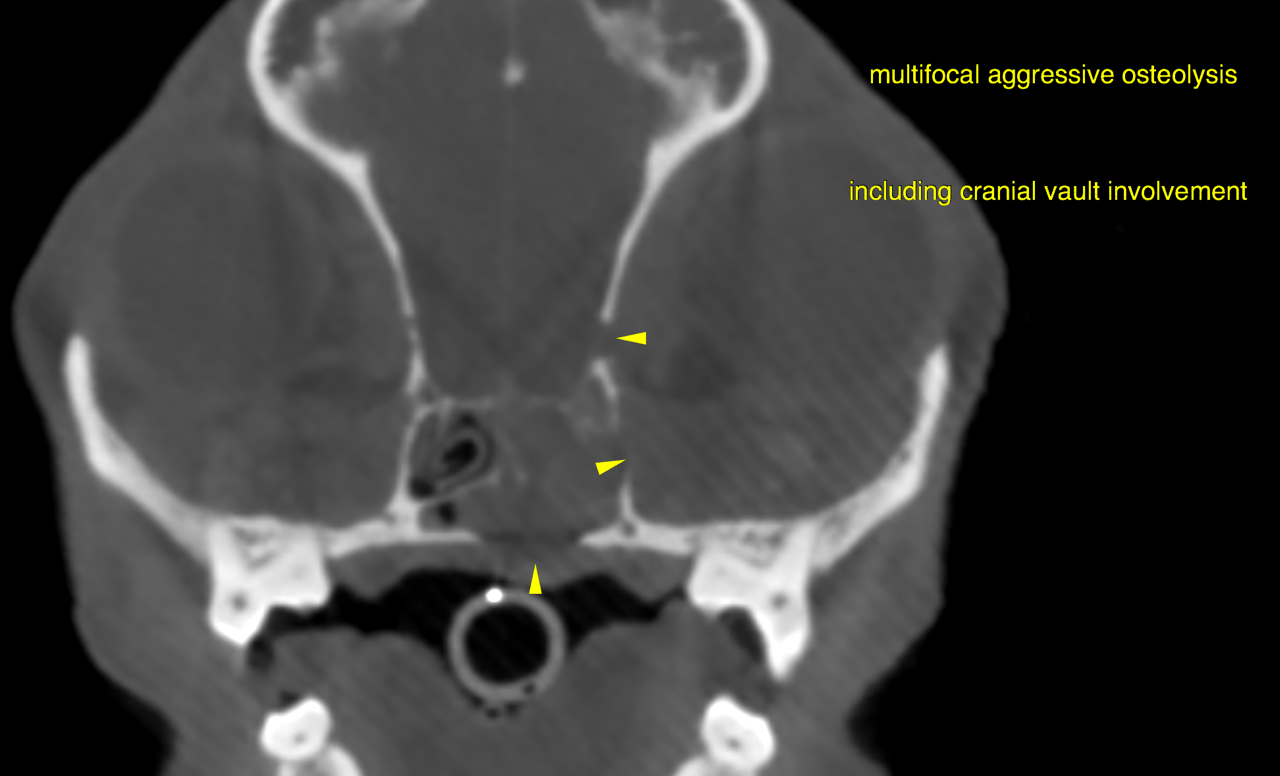
cavity. The nasal, palatinal, maxillary bones, bony nasal septum, bony orbita as well as
the hamulus of the pterygoidal bone and left-sided nasal turbinates present extensive
aggressive osteolysis emphasizing the mid and caudal third of the nasal cavities. The
mass penetrates into the right nasal cavity and the left orbita. There is a bony defect
within the frontal bone creating a connection with the cranial fossa. Actual tumor
growth inside the cranial fossa is not noted. The left frontal sinus is entirely filled with
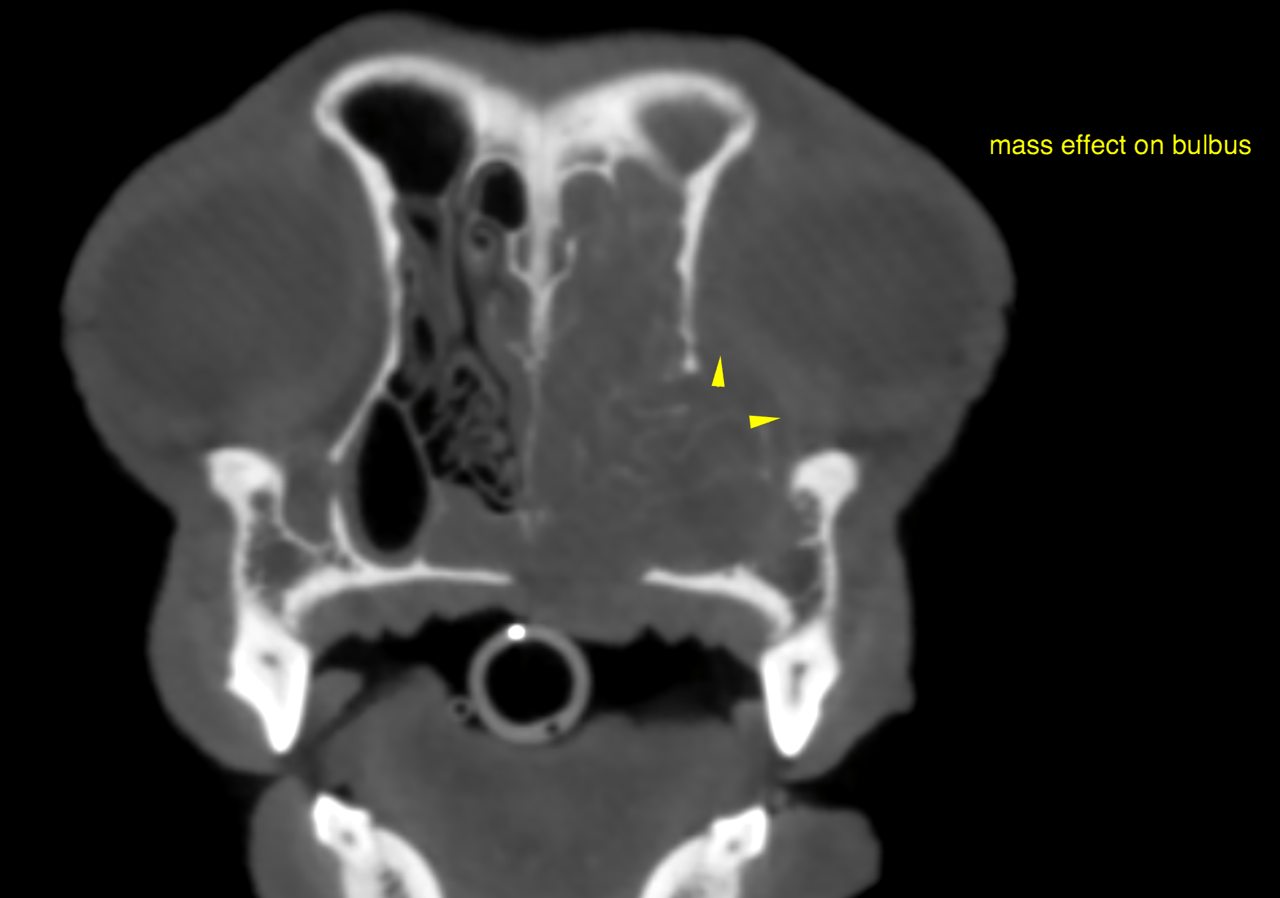
soft tissue attenuating material. A significant mass effect is exerted on the left bulbus,
which posterior pole is flattened and presents dorsotemporal deviation. A portion of
the mass is located within the nasopharynx and causes a significant left-sided and
central nasopharyngeal stenosis.
After administration of iodinated contrast there is moderate non-uniform enhancement
within the space-occupying lesion. The material within the frontal sinus does not show
contrast enhancement.
There are mild to moderate generalized signs of periodontal disease.
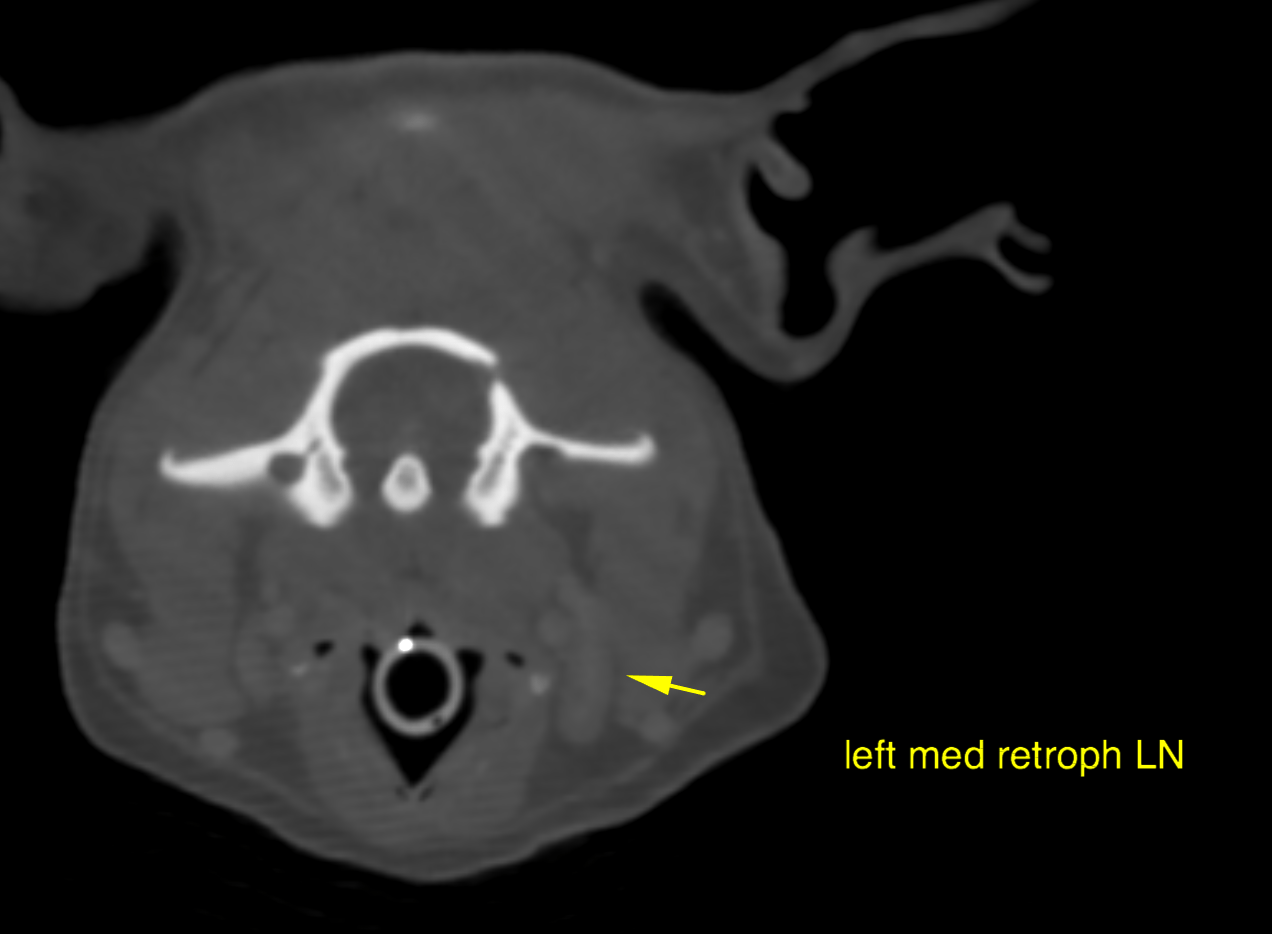
The left medial retropharyngeal lymph node presents moderate generalized
enlargement with preserved short-to-long axis ratio and contrast enhancement pattern.
The submandibular lymph nodes are within normal limits.
Likely differential
diagnoses include adenocarcinoma, squamous cell carcinoma, transitional cell
carcinoma, lymphosarcoma, melanoma, fibrosarcoma and other.
The computed tomographic findings do not meet the criteria of infectious destructive
rhinitis.
There is secondary secretory rhinitis and suspected metastatic spread to the left medial
retropharyngeal lymph node.
Palliative radiation therapy and/or chemotherapy may be considered after full tumor
staging (including tumor type diagnosis, 3 view chest radiographs, abdominal
ultrasound as well as fine needle aspiration of the left med. retropharyngeal lymph
node which may be accomplished under ultrasonographic guidance). Full surgical
resection – even radical hemimaxillectomy – is not an option here and even
cytoreductive surgery appears to be difficult.
Biopsy of mass done, results unavailable