A 9-year-old NM dog was presented for acute onset respiratory distress. A grade III/VI heart murmur was present on auscultation. radiographs revealed normal cardiac size and pulmonary vasculature with bonchoalveolar lung densities.
A 9-year-old NM dog was presented for acute onset respiratory distress. A grade III/VI heart murmur was present on auscultation. radiographs revealed normal cardiac size and pulmonary vasculature with bonchoalveolar lung densities.
Case Study
Acute Respiratory Distress Syndrome possible Pulmonary Thromboembolism (PTE) with Compenstaed Mitral Insufficiency and Prolapse in a Shih-tzu Dog. Stage B1 Valve Disease with non cardiogenic Pulmonary Consolidation.
Sonographic Differential Diagnosis
Sudden Acute Respiratory Distress Syndrome or pulmonary thromboembolic presentation. Mild LA enlargement. It is not felt to be the primary cause of the respiratory episode. Early pulmonary hypertension. This patient is at high risk for sudden death. Oxygen, blood pressure, bronchodilator, Torbutrol and Lasix therapy would be warranted as well as cage rest. Aspirin or plavix therapy can be considered. A recheck is recommended in 7-10 days. 24 hour care is highly encouraged.
Image Interpretation
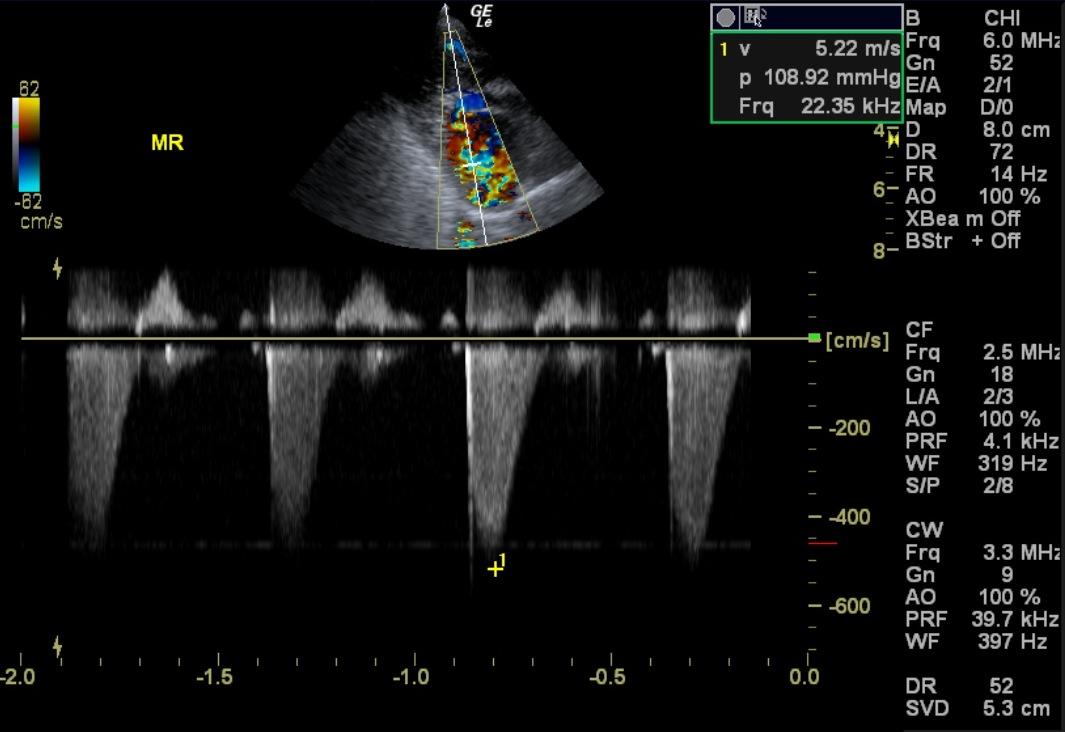
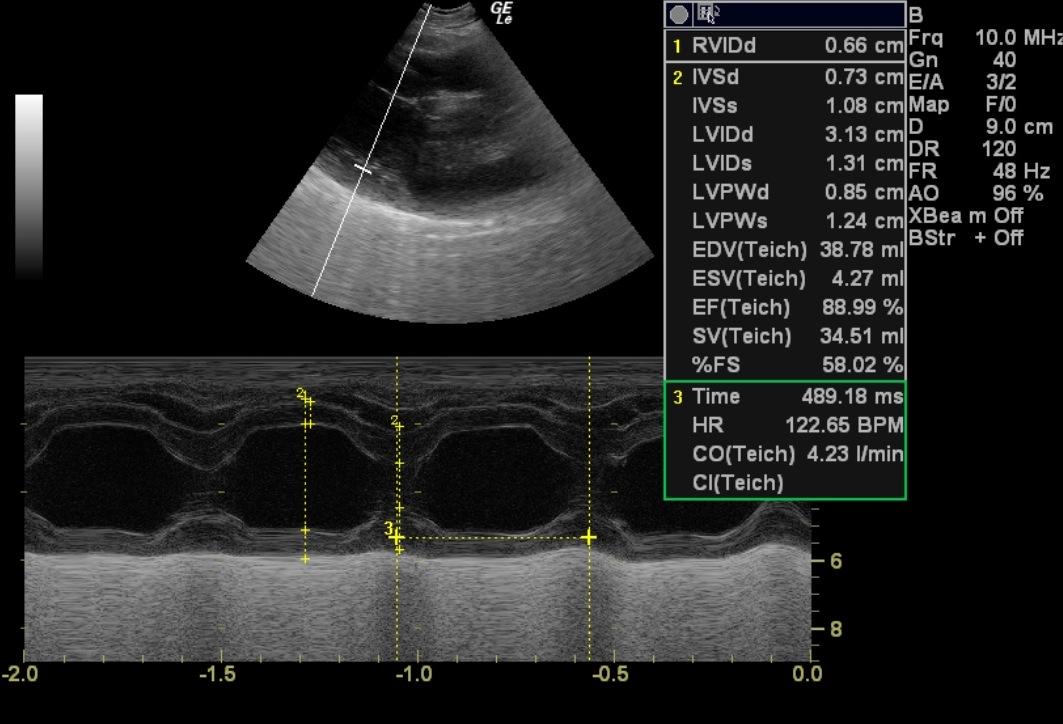
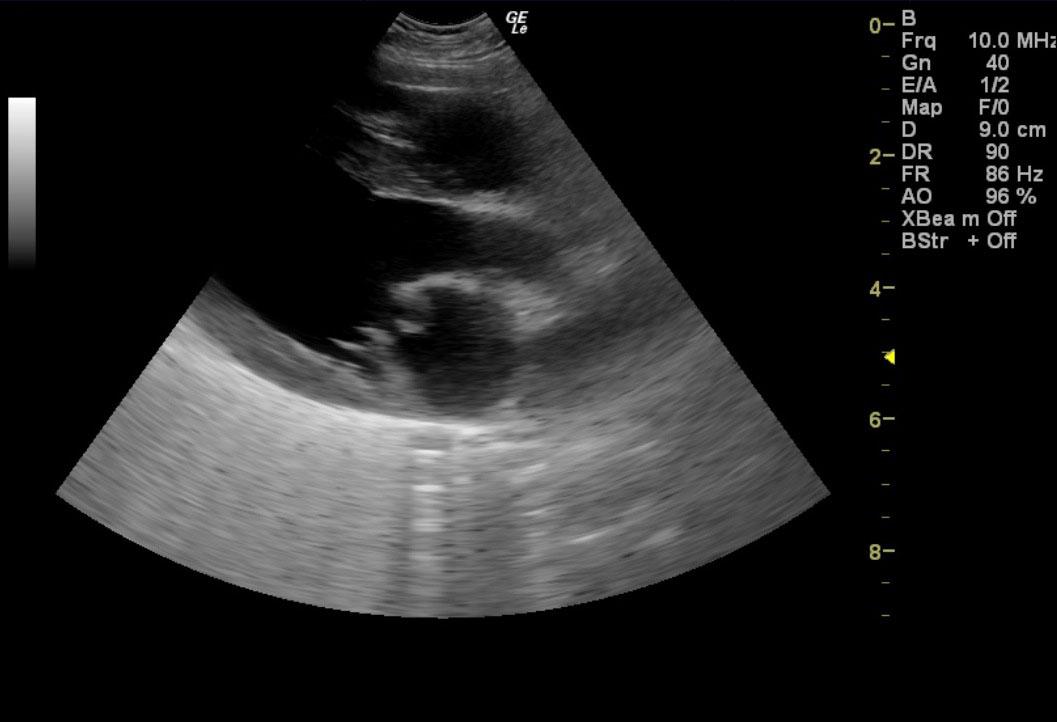
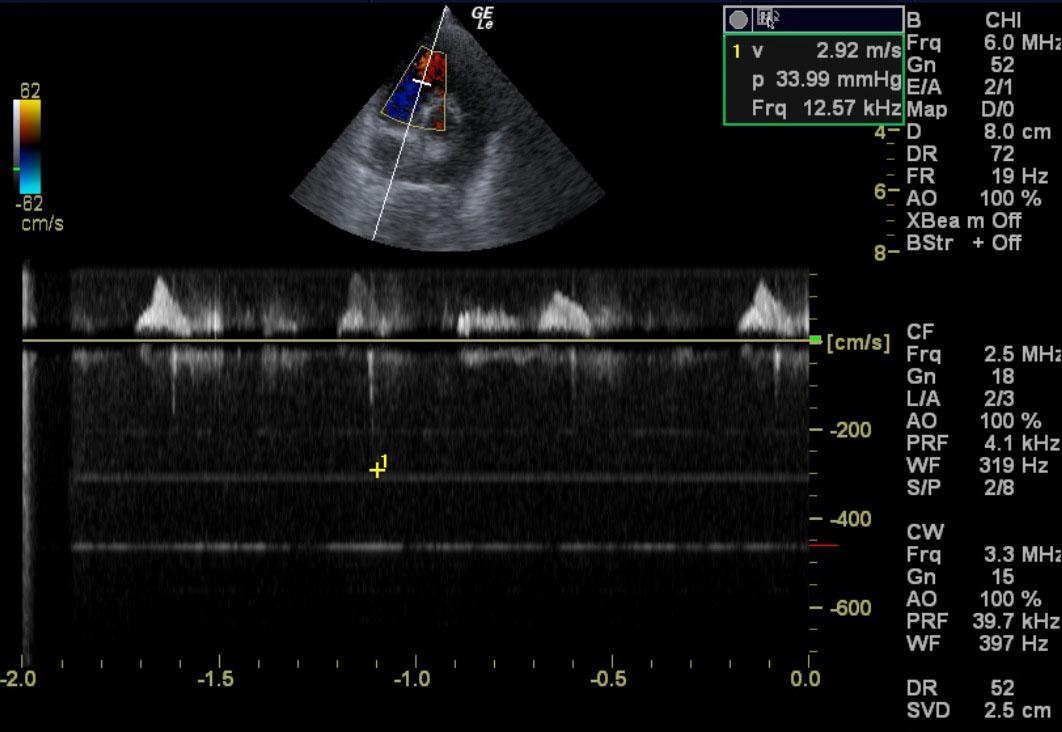
Rapid examination was performed of the thorax owing to respiratory distress. The echocardiogram for this patient presented a left atrium of slightly excessive size with anechoic content as did the corresponding LA:AO ratio. It is felt that left sided heart disease may be contributing, but is not the primary cause of the pulmonary pattern in this patient. No evidence of “smoke” or thrombotic activity was noted. The cranial and caudal mitral valve leaflets demonstrated mildly vegetative contour. End point to septal separation was within normal limits as the cranial leaflet came in contact or adequately close to the ventricular septum upon systolic motion. The left ventricle demonstrated prominent volume, normal septal and free wall diastolic thicknesses, and papillary integrity. Ventricular function was deemed adequate to hyperdynamic expressed by the fractional shortening measurement. The right atrium was subjectively assessed and found to be uniformly smaller than the left atrium without evidence of dilation or contraction. No neoplastic evidence was visualized here or into its extension of the right auricle. The tricuspid valve revealed insufficiency consistent with mild early pulmonary hypertension. The right ventricle demonstrated normal size (1/3 diameter of the left ventricle), morphology, and kinetic activity. No evidence of heartworm or infiltrative disease was noted. The pulmonic outflow tract presented free of dilation (1:1 PA/AO ratio), adequate laminar flow, no evidence of insufficiency, and free of visible heartworm activity. The myocardium throughout the heart was uniformly echogenic without evidence of significant fibrosis, infiltrative disease (lymphoma, hemangiosarcoma) or ischemic events (infarcts). Diffuse, shower curtain pattern was noted throughout the alveolar and bronchi in the extra cardiac space. This is consistent with acute respiratory distress syndrome and thromboembolic disease. Given the acute onset SARDS or pulmonary thromboembolic disease is suspected. Mitral insufficiency 5.2 m/sec. Tricuspid insufficiency 2.8 m/sec.
Outcome
The patient was euthanized owing to lack of response to therapy (lasix, oxygen, sedation, cage rest, and economic issues
Comments
The Shih-tzu and Maltese breeds of geriatric age are overrepresented in this type of SARDS syndrome in our archive
Clinical Differential Diagnosis
Respiratory – acute pneumonia, edema, SARDS, embolic disease, pulmonary hypertension, lobe torsion Pleural effusion. Cardiac – mitral valve endocardiosis/endocarditis, ruptured chordae tendinae, myocardial failure, cardiomyopathy (dilated/hypertrophic), pericardial effusion with tamponade.
Sampling
None
Video
Patient Information
Patient Name :
Lucky K
Gender :
Male, Neutered
Species :
Canine
Type of Imaging : Ultrasound
Book :
yes
Status :
Complete
Liz Wuz Here :
Yes
Code :
15-00121
Clinical Signs
- Dyspnea
Exam Finding
- Heart Murmur
Images
Clinical Signs
- Dyspnea