A 13-year-old MN Pomeranian was presented for evaluation of a cardiac murmur. There was history of coughing and survey radiographs were within normal limits.
A 13-year-old MN Pomeranian was presented for evaluation of a cardiac murmur. There was history of coughing and survey radiographs were within normal limits.
Case Study
15_00079 Pee Wee M Severe pulmonary hypertension-
Sonographic Differential Diagnosis
This patient suffers from severe pulmonary hypertension. Main causes for this pathology are heartworms, pulmonary fibrosis, pulmonary thromboembolism, shunting or congestive heart failure. Thromboembolism can be a sequelae of hyperadrenocorticism, trauma, tumor or nephrotic syndrome (to mention the most probable causes). Heartworm antigen should be checked even though there are no adult worms seen on the echo. The findings can of course explain the symptoms described.
Image Interpretation
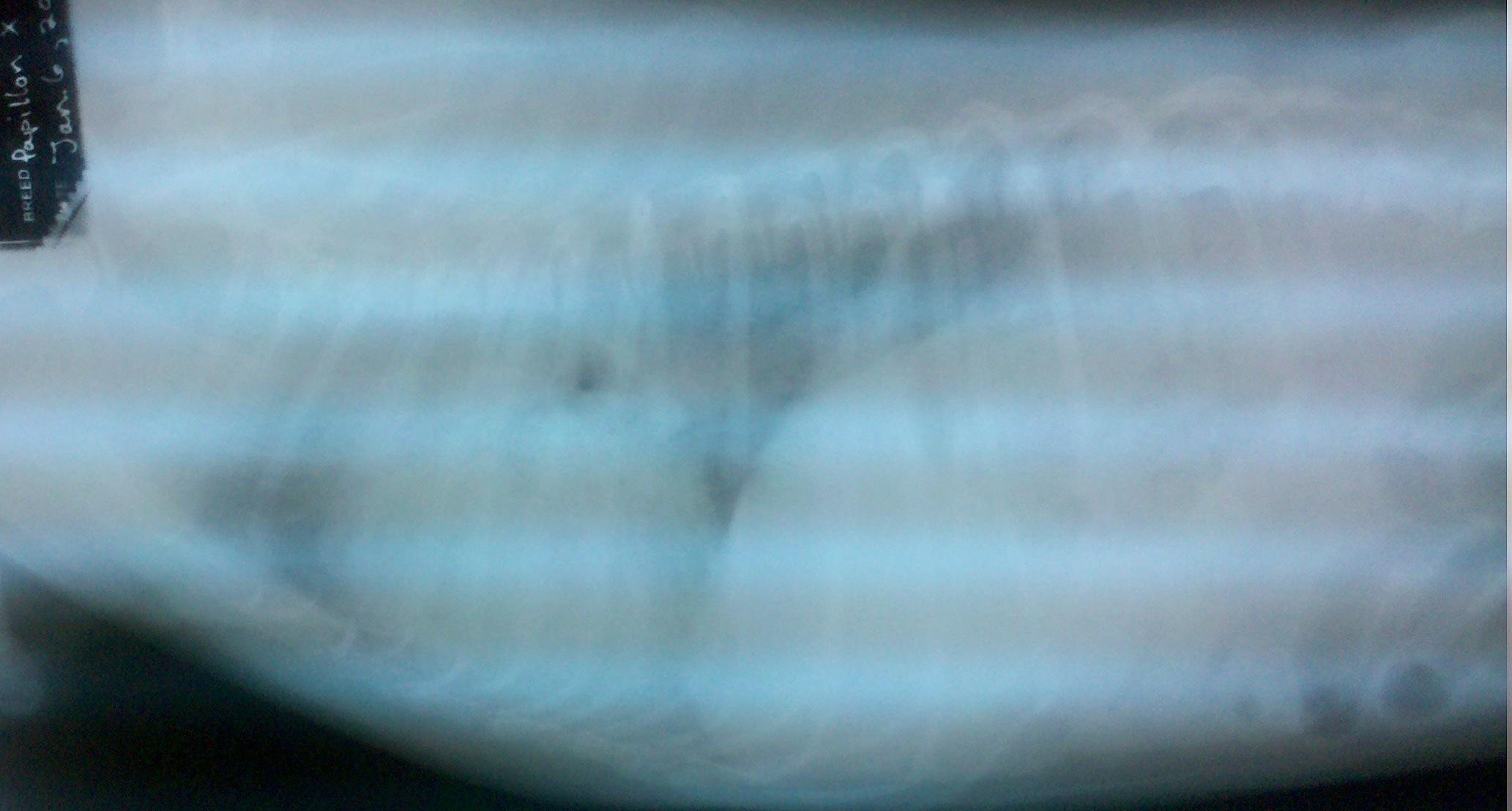
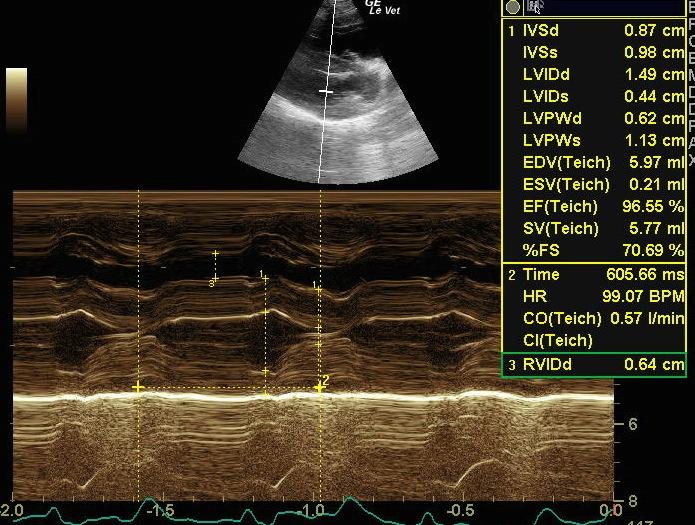
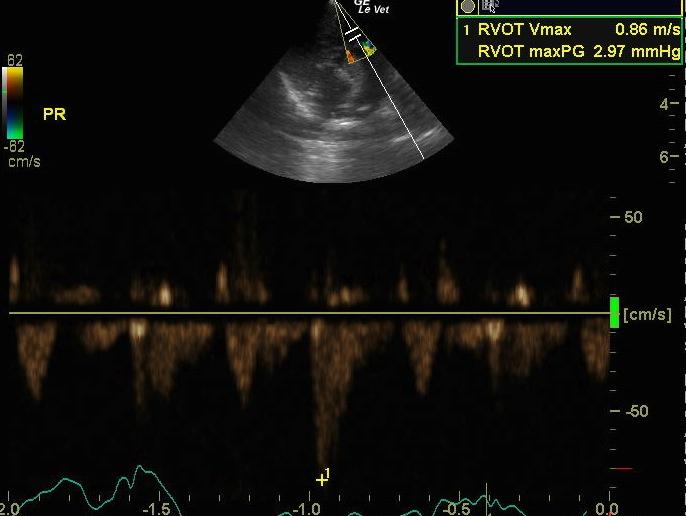
The radiographs show clear evidence of massive right heart enlargement and (as far as visible on the photographs) a marked interstitial lung pattern. The left ventricle and atrium are normal sized. The caudal vena cava is markedly enlarged. There is a volume depleted and pseudo hypertrophied left ventricle and a merely tiny left atrium. The right ventricle is severely hypertrophied, the right atrium is severely enlarged. The mitral valve is mildly thickened, the tricuspid valve is morphologically normal but pressed into the right atrium during systole. Flow across the LVOT is normal ruling out any stenosis and supporting the theory that the left ventricular hypertrophy is only due to volume depletion (pseudo-hypertrophy). Flow across the RVOT shows clearly an asymmetric flow profile (characteristic of pulmonary hypertension) but a normal maximal velocity. There is moderate tricuspid insufficiency and mild pulmonary insufficiency present. TI has a maximal velocity of 4,6 m/s, indicating a systolic pulmonary arterial pressure of at least 90 mm Hg. The pulmonary insufficiency profile shows a vmax of 4 m/s, so mean pulmonary pressure has to be at least 64 mm Hg.
DX
Severe pulmonary hypertension
Comments
I would treat the patient with Sildenafil (1-2 mg/kg bid), Pimobendan, aspirin and propentofylline. You should not expect a marked reduction of the TI pressure gradient but the owner should notice clinical improvement of the patient. Prognosis is usually guarded in such patient.
Clinical Differential Diagnosis
Cardiac – mitral/tricuspid endocardiosis, vegetative endocarditis, myocardial weakness, heartworm disease. Anemia.
Sampling
None
Video
Patient Information
Gender :
Male, Neutered
Species :
Canine
Type of Imaging : Ultrasound
Status :
Complete
Clinical Signs
- Coughing
- Heart Murmur
Images

Clinical Signs
- Coughing
- Heart Murmur