An 11-year-old NM canine mix with a history of surgery for foreign body ingestion was presented for evaluation of progressive intermittent vomiting. cPL was normal.
An 11-year-old NM canine mix with a history of surgery for foreign body ingestion was presented for evaluation of progressive intermittent vomiting. cPL was normal.
Jejunal foreign matter obstruction with primary dysfunctional bowel. Transmural bowel necrosis with potential for underlying focal lymphoma or carcinoma is less likely. It appears resectable. The hope is that only an inflammatory bowel type event is present in this patient without evident neoplasia. However, with loss of mural detail associated with the foreign matter I am concerned for primary disease as well as secondary degenerative disease from embedded material. Corn cob or similar consistency would fit with the sonographic properties of the luminal material. Given the periserosal inflammatory pattern, this indicates transmural inflammation. Resection and anastamosis ideally guided by intraoperative ultrasound would be the best approach in this case to fully resect the affected bowel.
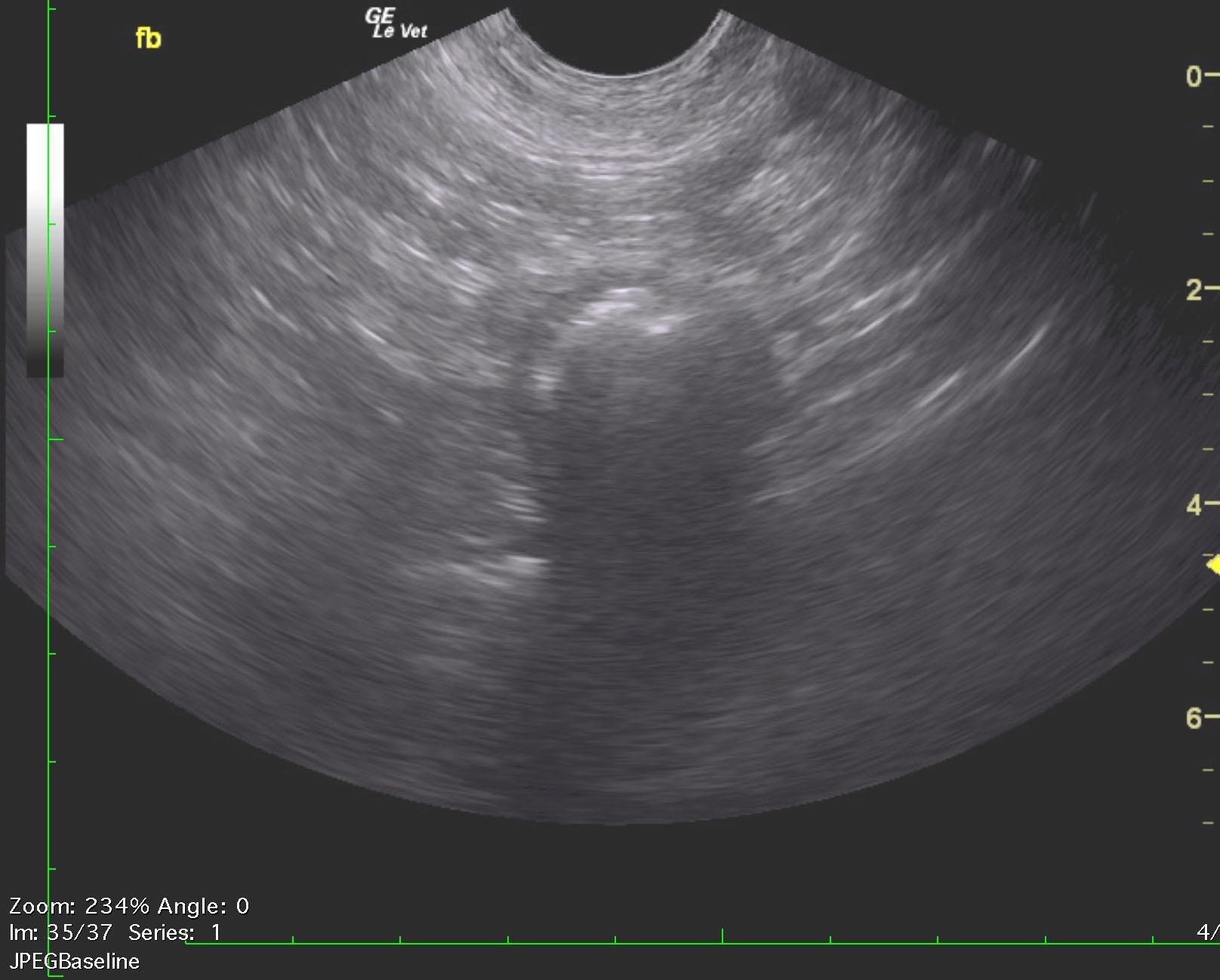
The upper gastrointestinal tract was unremarkable. The mid jejunum revealed a 2.5 cm shadowing luminal structure with hypertrophy of the regional bowel and some loss of detail with minor periserosal inflammatory pattern. This is likely foreign matter embedded within primary mural disease of the intestine. Recommend immediate resection and anastomosis along with removal of the foreign matter embedded within the intestine. Intraoperative ultrasound to fully delineate the detail loss within the wall of the intestine is strongly recommended in this case.
None
GIT – IBD, neoplasia, foreign body, intussusception, dietary hypersensitivity
Focal peritonitis
None