A 13-year-old Shepherd mix was presented for evaluation of acute onset vomiting, diarrhea, and pyrexia.
A 13-year-old Shepherd mix was presented for evaluation of acute onset vomiting, diarrhea, and pyrexia.
Intestinal necrosis pattern with regional peritonitis.
Slight free fluid.
Loss of bowel detail, concurrent colitis, potential underlying intestinal lymphoma or mast cell disease. Spontaneous necrosis and inflammatory bowel is likely with potential septic mural penetration. Aggressive antibiotics such as Enrofloxacin and Metronidazole combination, plasma expansion and aggressive fluid therapy are recommended over the next 48-72 hours while cytology is being evaluated. A recheck sonogram is recommended in 4-5 days or earlier if clinical signs continue to deteriorate. Guarded prognosis.
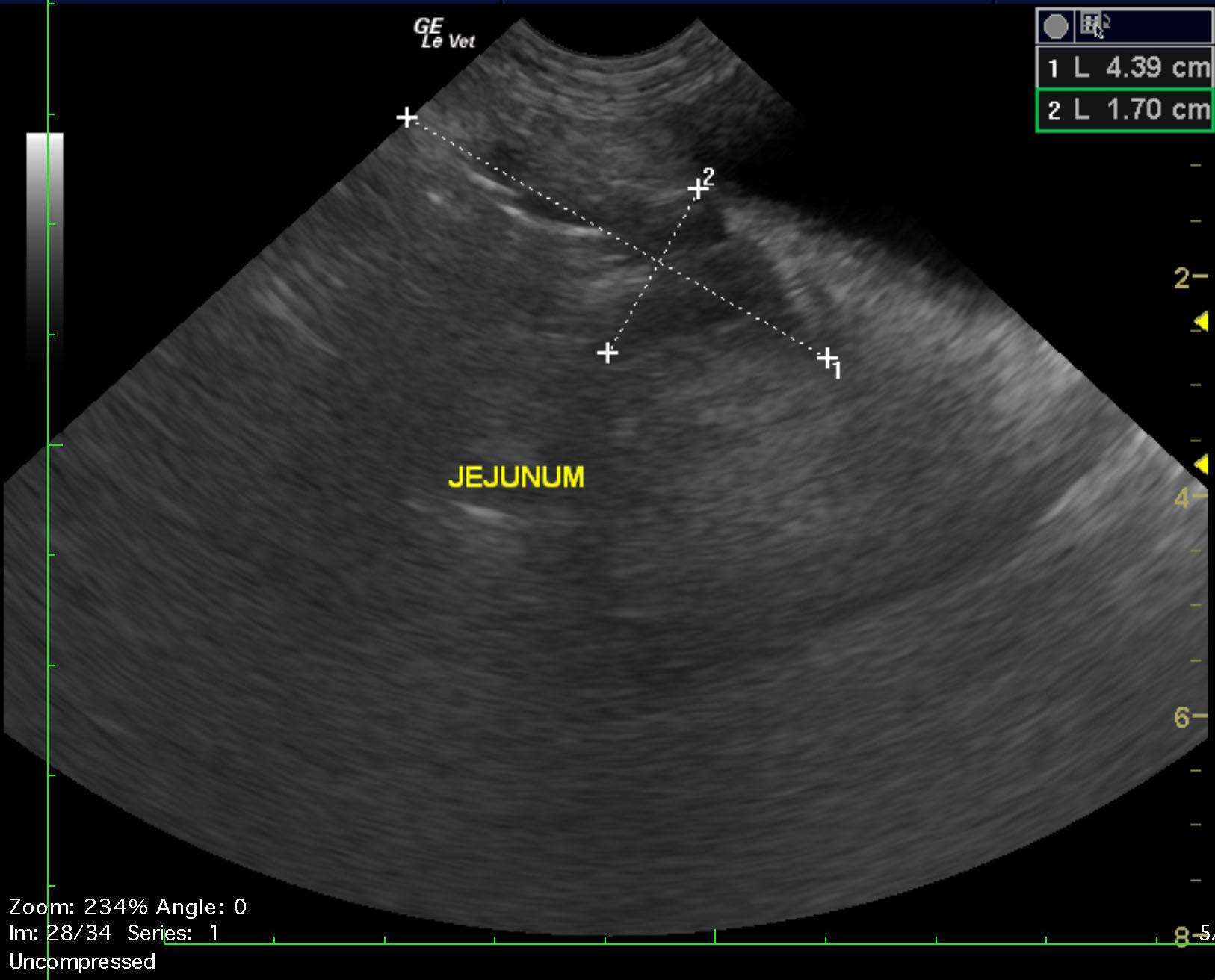
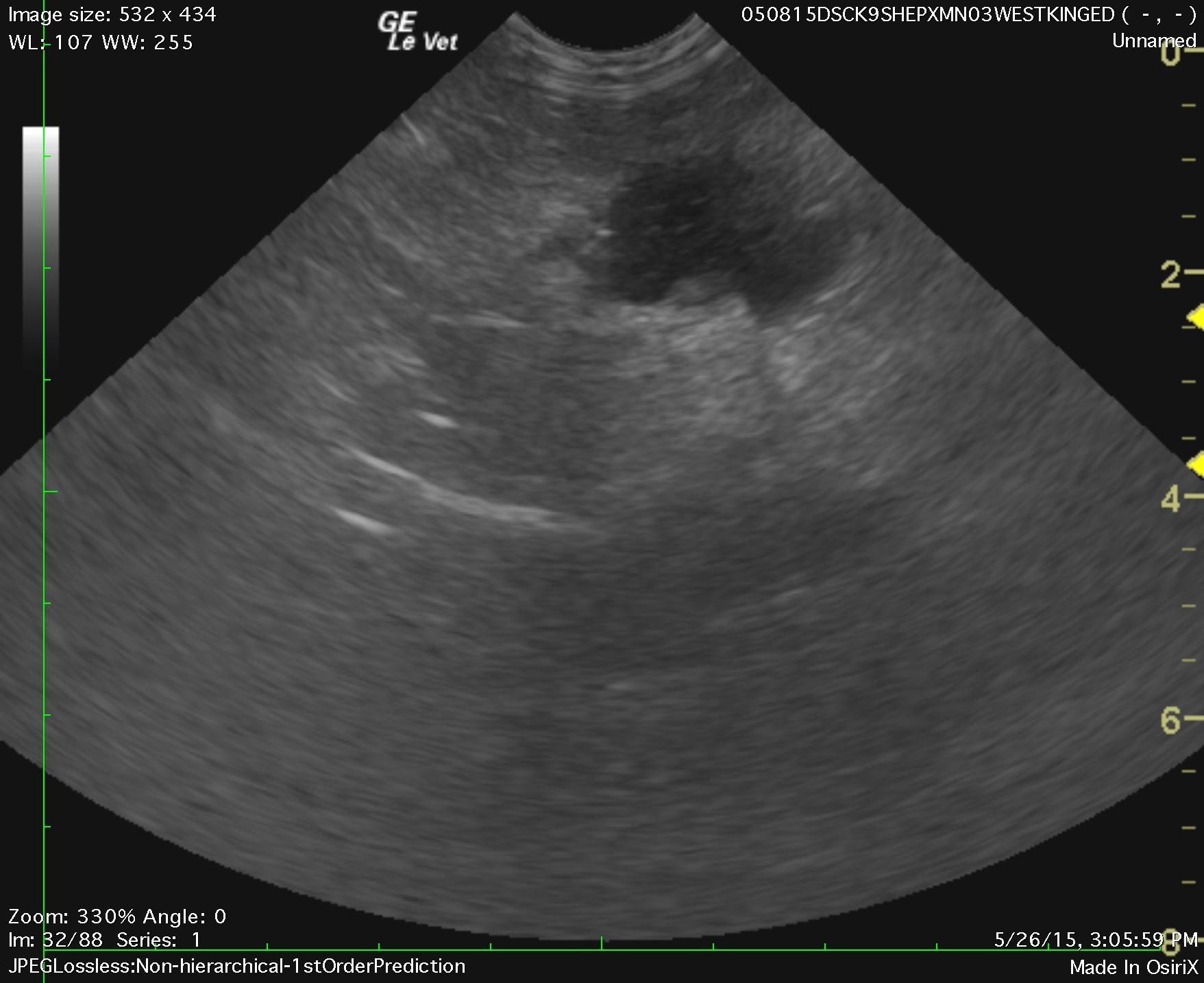
The upper gastrointestinal tract appeared relatively unremarkable. However, the distal small intestine and colon were significantly thickened. A portion of the distal jejunum or ileum close to the ileocecal region revealed focal, regional, mixed hypoechoic lesion with reactive surrounding fat. A separate portion of jejunum was thickened and spasmic with loss of detail and measured 4.39 x 1.7 cm and had regional inflammation with echogenic material and corrugated bowel. The colonic wall measured 0.6 cm. Ill defined mesentery was noted from the ileocecal region to the urinary bladder. A portion of intestinal pathology adjacent to the ileocecal valve measured 2.38 x 1.8 cm. Ultrasound-guided FNAs were performed of this lesion without complication.
None
GIT – obstruction, torsion, ulceration, focal perforation with peritonitis
Pancreas – pancreatitis
Peritonitis
Liver – acute hepatitis (viral, bacterial, toxins), neoplasia, abscess, granulomatous disease
Gall bladder – cholecystitis, mucocele
Culture of the jejunum grew Streptococcus canis, Beta strep. Group G and Escherichia coli. Cytology of the jejunum was inconclusive, +/- slight neutrophilic inflammation.