A 2-year-old MI Pug was presented for not urinating, lethargy, and one episode of vomiting. On physical examination the urinary bladder was distended and could not be expressed. An attempt was made to place a urinary catheter, but an obstruction was encountered at the base of the os penis. An 8 French urinary catheter was successfully placed after flushing with saline and was left as an in-dwelling catheter. The urine had a cloudy appearance and on urinalysis showed elevated pH, 3+ bilirubinuria, 4+ urobilinogen, and hematuria.
A 2-year-old MI Pug was presented for not urinating, lethargy, and one episode of vomiting. On physical examination the urinary bladder was distended and could not be expressed. An attempt was made to place a urinary catheter, but an obstruction was encountered at the base of the os penis. An 8 French urinary catheter was successfully placed after flushing with saline and was left as an in-dwelling catheter. The urine had a cloudy appearance and on urinalysis showed elevated pH, 3+ bilirubinuria, 4+ urobilinogen, and hematuria. CBC was within normal limits, whereas abnormalities on blood chemistry were low BUN, elevated ALT and elevated ALP activity, hypocholesterolemia, hypoamylasemia, and respiratory alkalosis (high pH and low PCO2. The patient was treated with Amoxicillin, Famotidine, and Pepcid. Recheck blood work 24 hours later showed low BUN, low total protein, but a reduction in the ALT and a reduction in ALP activity.
Case Study
03_00177 Loki E Portosystemic shunt
Sonographic Differential Diagnosis
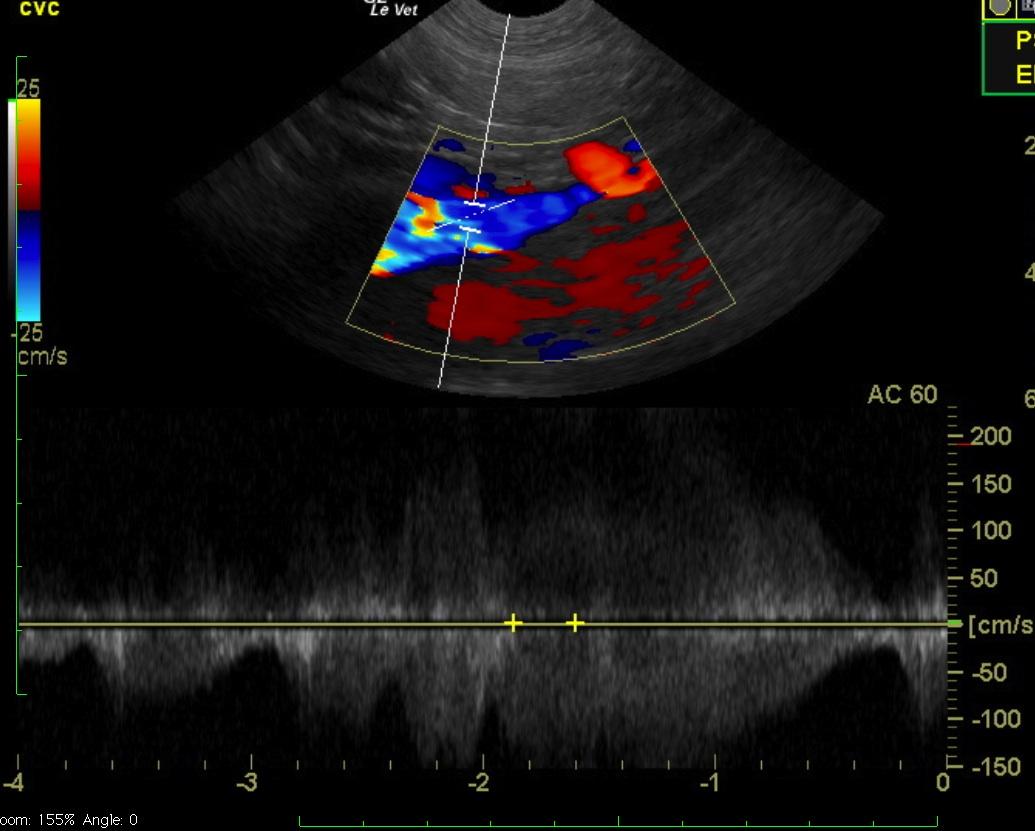
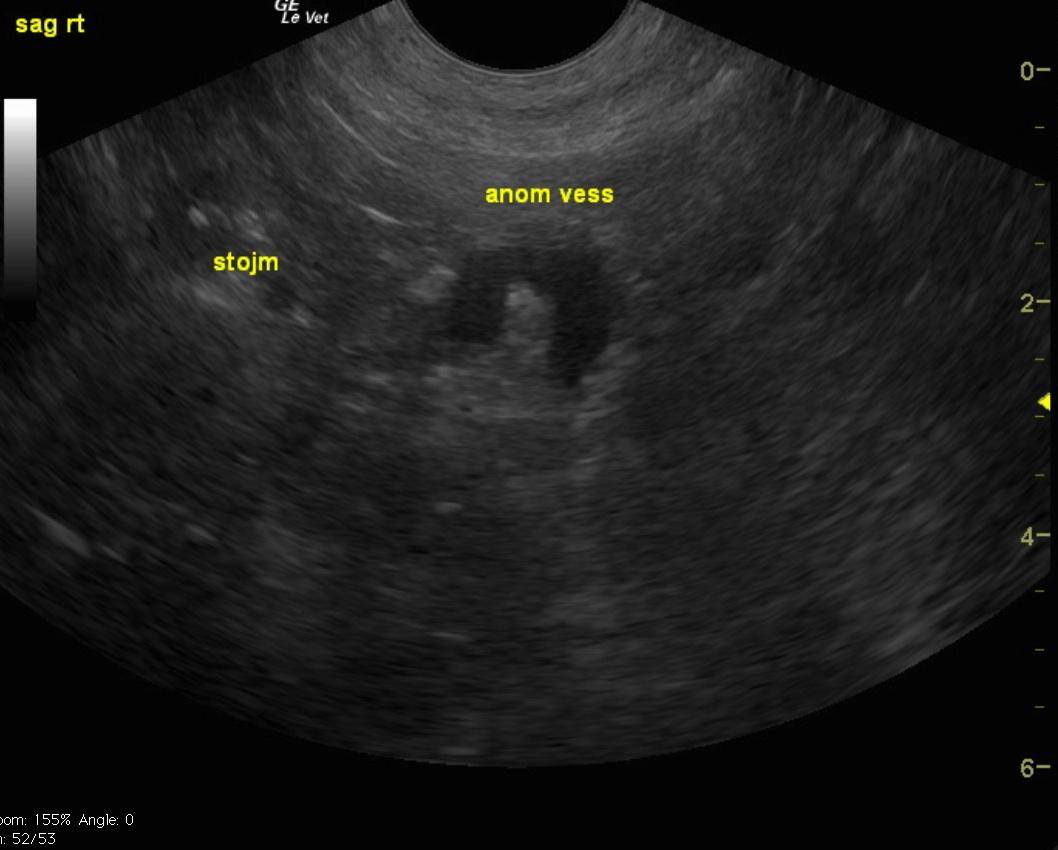
Microhepatica and extrahepatic portosystemic shunt. Given the contour and direction gastrocaval shunt likely.
Image Interpretation
The liver is visibly subnormal in size. A large tortuous extrahepatic vessel is noted directed toward the transducer in a ventral direction indicated in red, then turning and directed dorsally away from the transducer in blue. The vessel continues dorsally into the region of the vena cava or potentially bypassing the vena cava and entering the azygos vein into the thorax. However, given the significant turbulence in the CVC noted on CF and PW Doppler the aberrant vessel enters into the vena cava.
DX
Outcome
The owner was discussing options for surgery at last follow-up.
Clinical Differential Diagnosis
Bladder obstruction – urolith, blood clot, prostatic disease (hypertrophy, prostatitis, abscessation), urethra (urolith, urethratitis, polyp.) Liver – acute liver disease (toxins, infectious, trauma), congenital (PSS, MVD.)
Video
Patient Information
Clinical Signs
- Dysuria
- Lethargy
- Not Urinating
- Vomiting
Images

Blood Chemistry
- Alkaline Phosphatase (SAP), High
- ALT (SGPT), High
- BUN low
- Cholesterol, Low
Clinical Signs
- Dysuria
- Lethargy
- Not Urinating
- Vomiting
Urinalysi
- Appearance Turbid
- Bilirubin Present
- Blood Present
- pH High