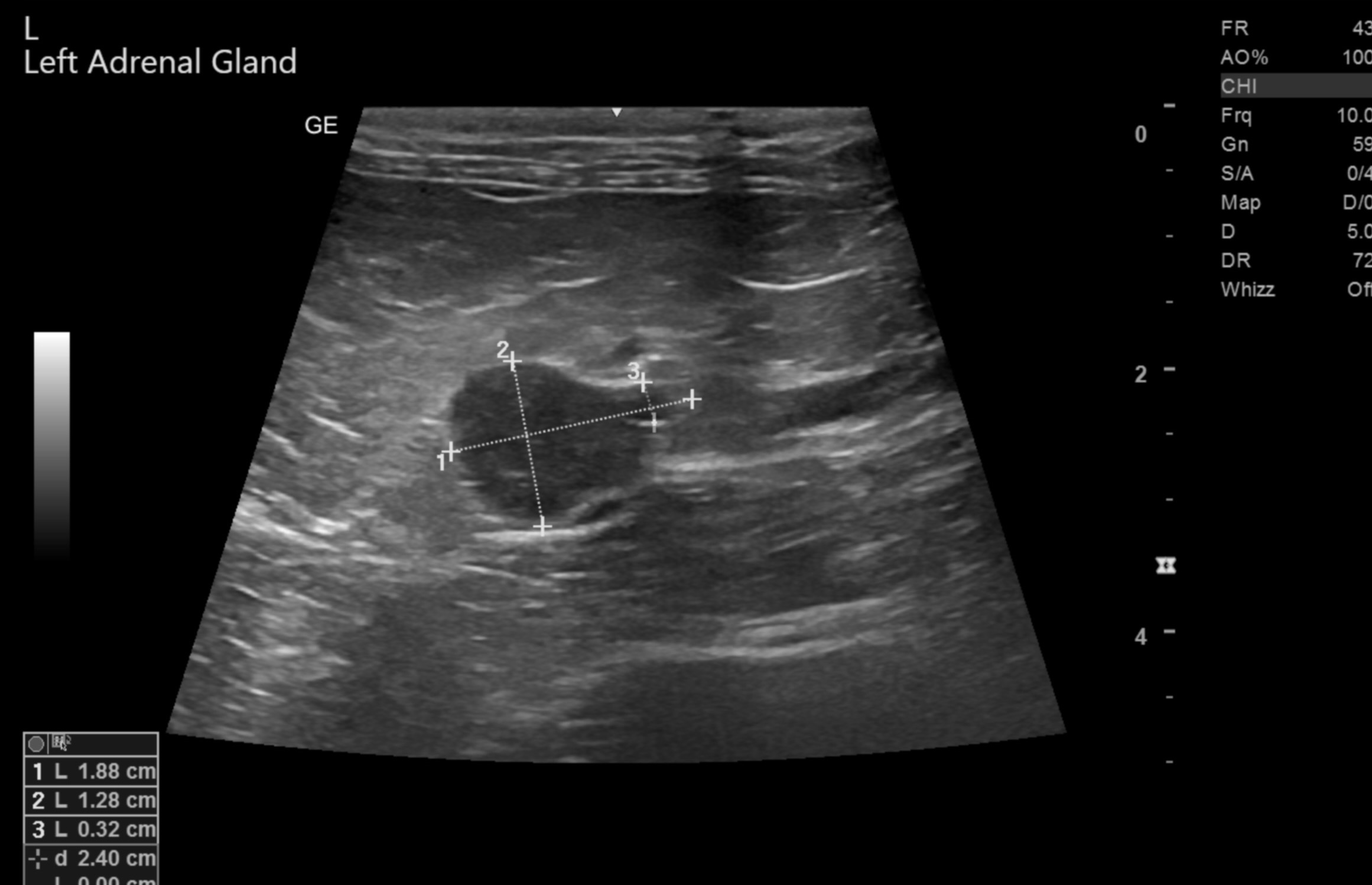
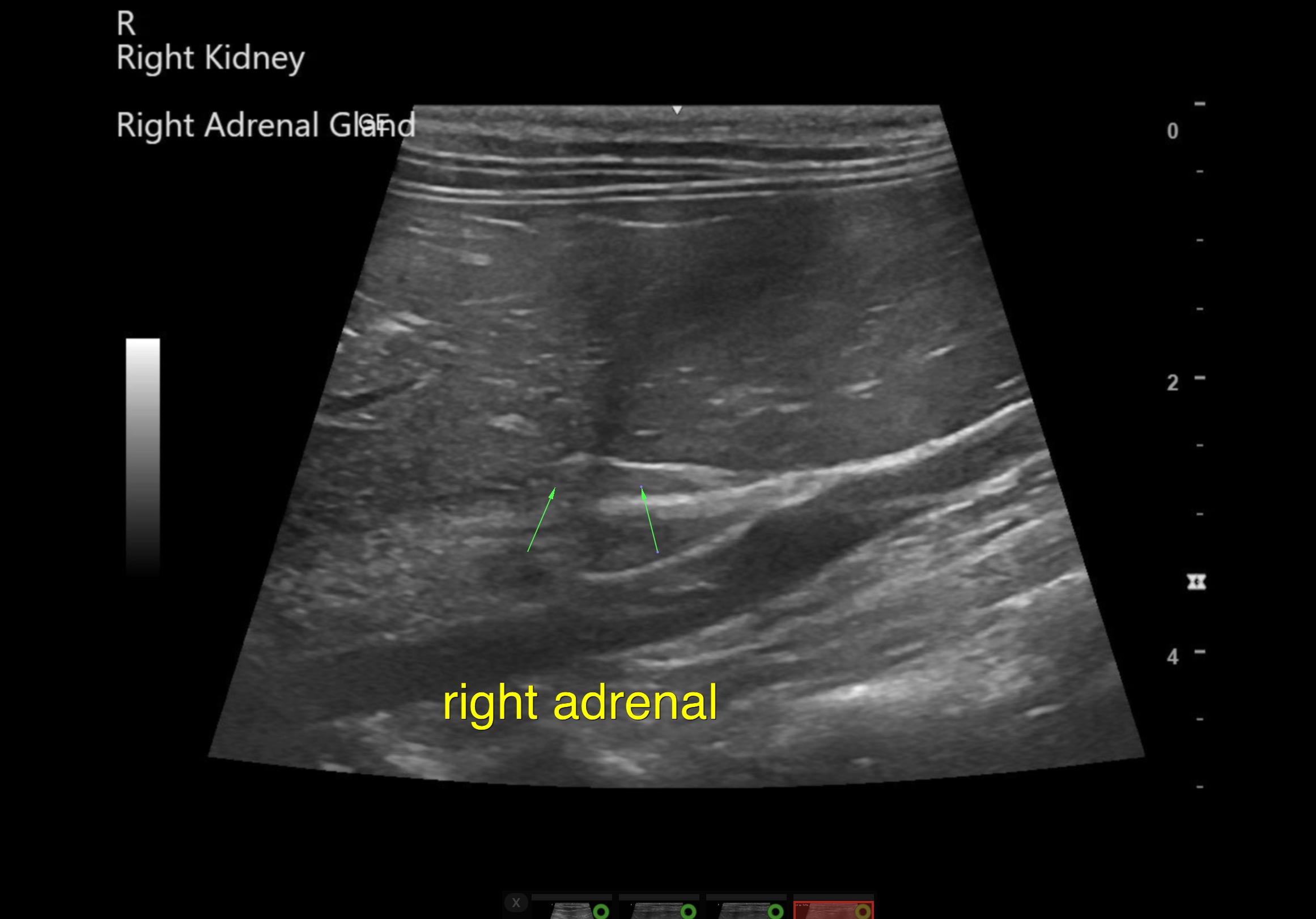
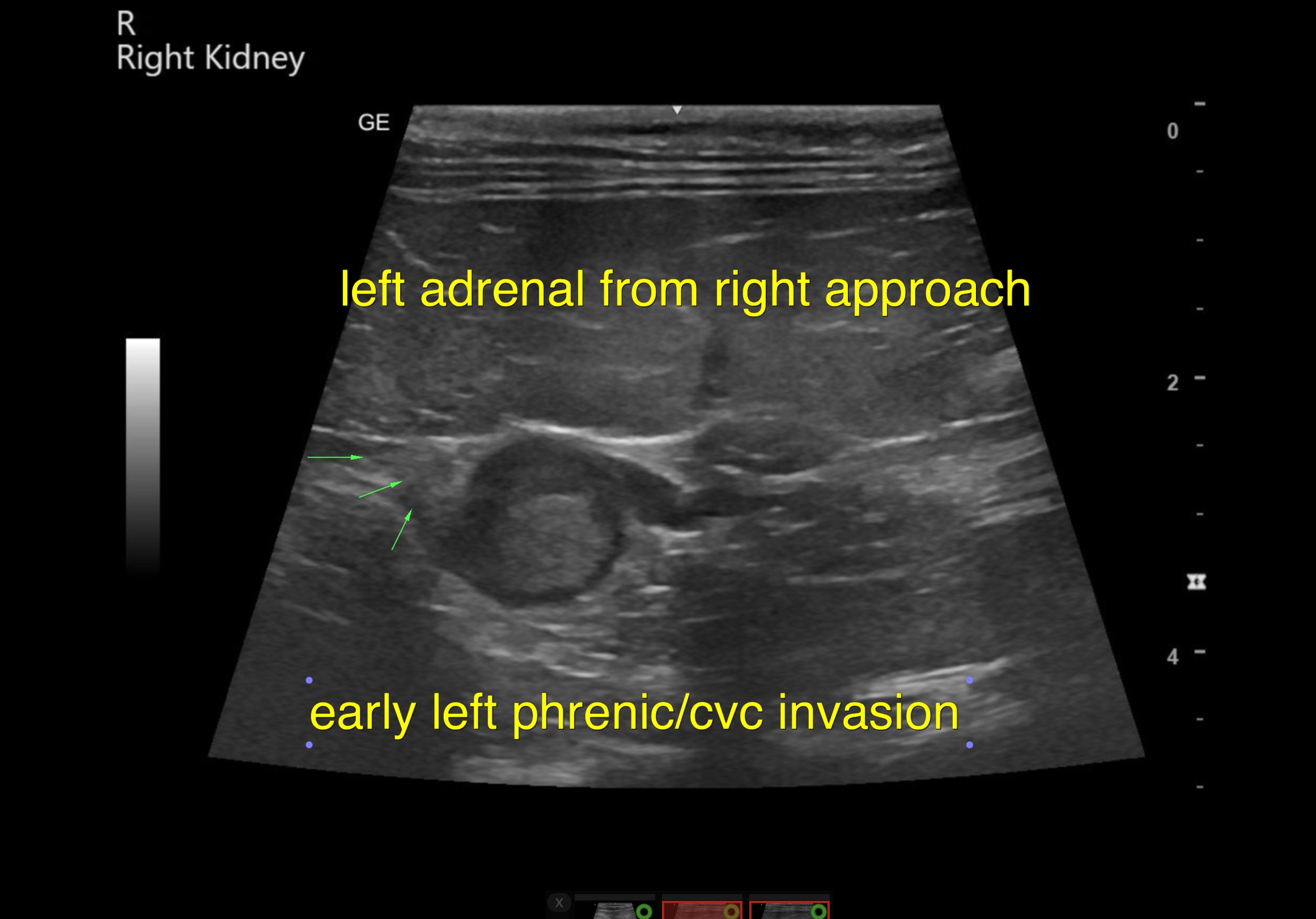
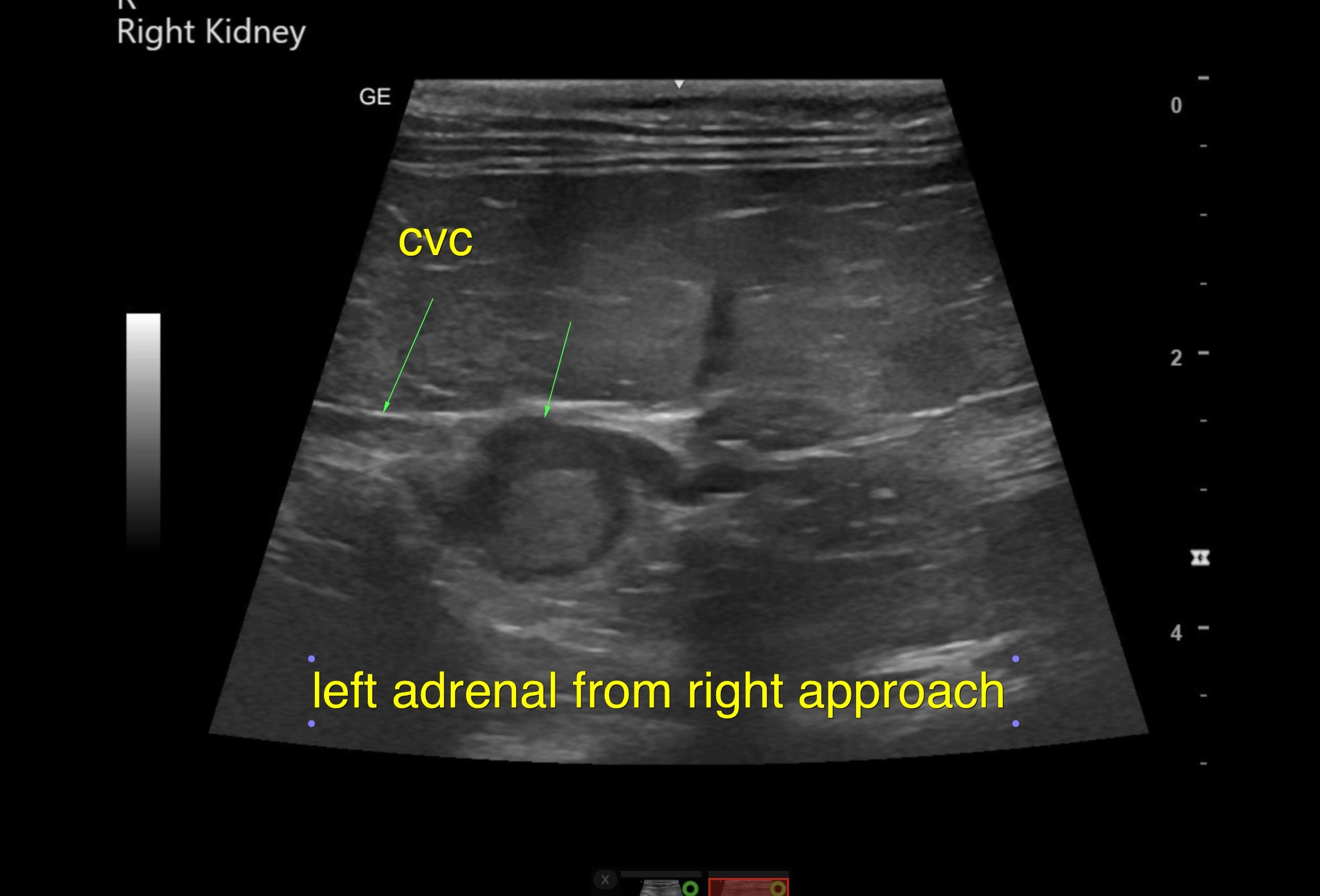
The left adrenal gland was enlarged, rounded, and hypoechoic to surrounding fat. The left adrenal measured 1.88cm x 1.2 cm at the cranial pole and 0.32 cm at the caudal pole. Upon the right approach to the left adrenal mass, visualizing the vena cava and phrenic vein, an early invasion appears to be present – extending approximately 7.0 mm into the phrenic vein and vena cava. The right adrenal gland measured3.0 mm in width, not pathological.
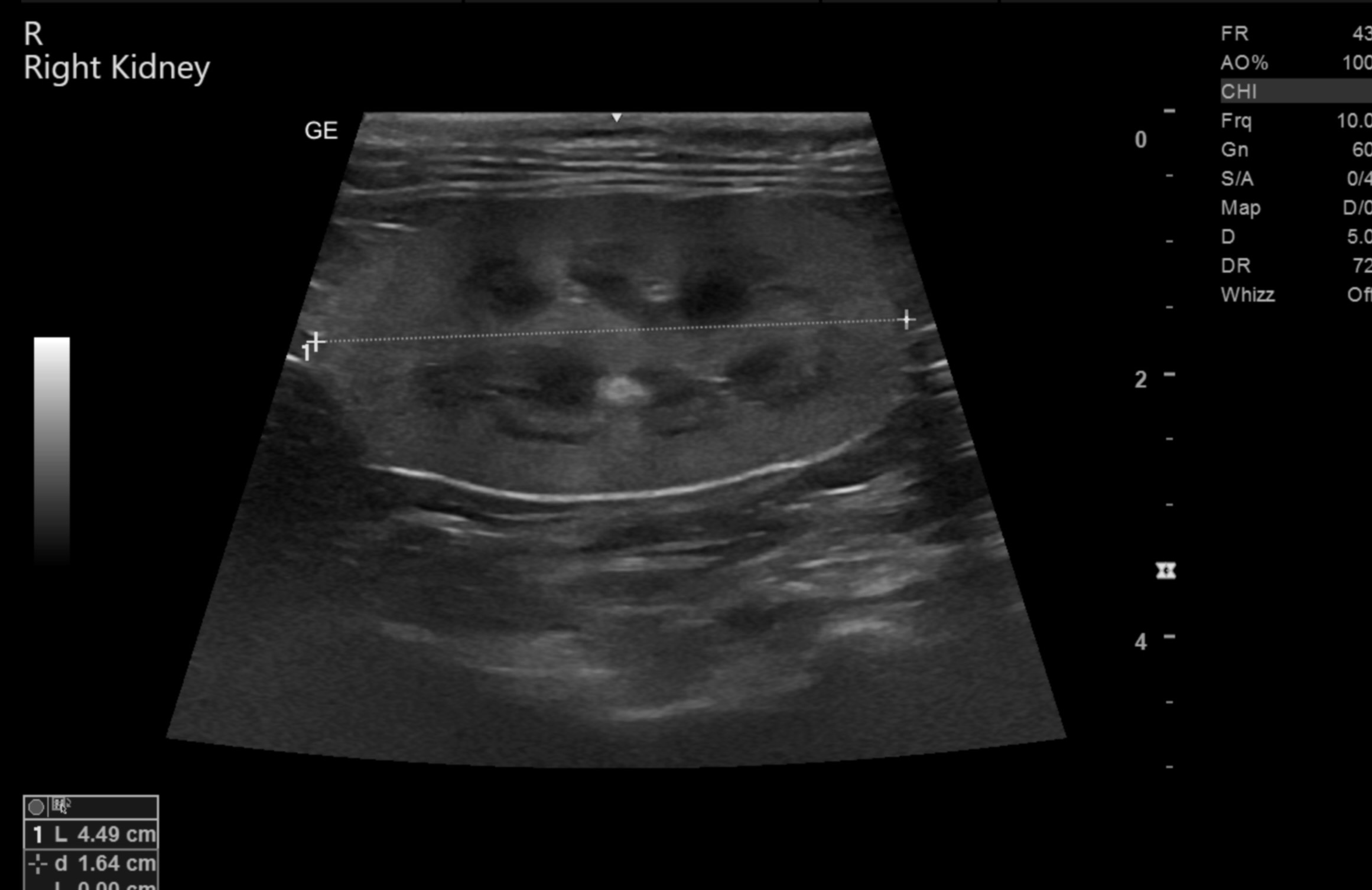
The kidneys were normal in size and contour with slight hypoechoic idiopathic medullary rim.