This 11 year old MN beagle dog presented with a chronic cough
This 11 year old MN beagle dog presented with a chronic cough
This 11 year old MN beagle dog presented with a chronic cough
This 11 year old MN beagle dog presented with a chronic cough
CT of the thorax, plain and post contrast – The lungs are expanded. There is multifocal cylindrical peripheral bronchiectasis with
uneven diameter of the bronchi. Accumulations of pulmonary secretions within the
affected bronchi are not noted, the bronchial walls are not thickened. A mild and
symmetrical subpleural interstitial ground glass opacity is noted in the dorsal aspect of
both caudal lung lobes.
The mediastinal lymph nodes are prominent but present with regular architecture,
attenuation and enhancement pattern.
The overall size of the heart and the volume relationships of the cardiac chambers are
within normal limits (see pictures below). No abnormalities of the major vessels are
detected. There is no evidence of pulmonary venous or arterial hypertension.
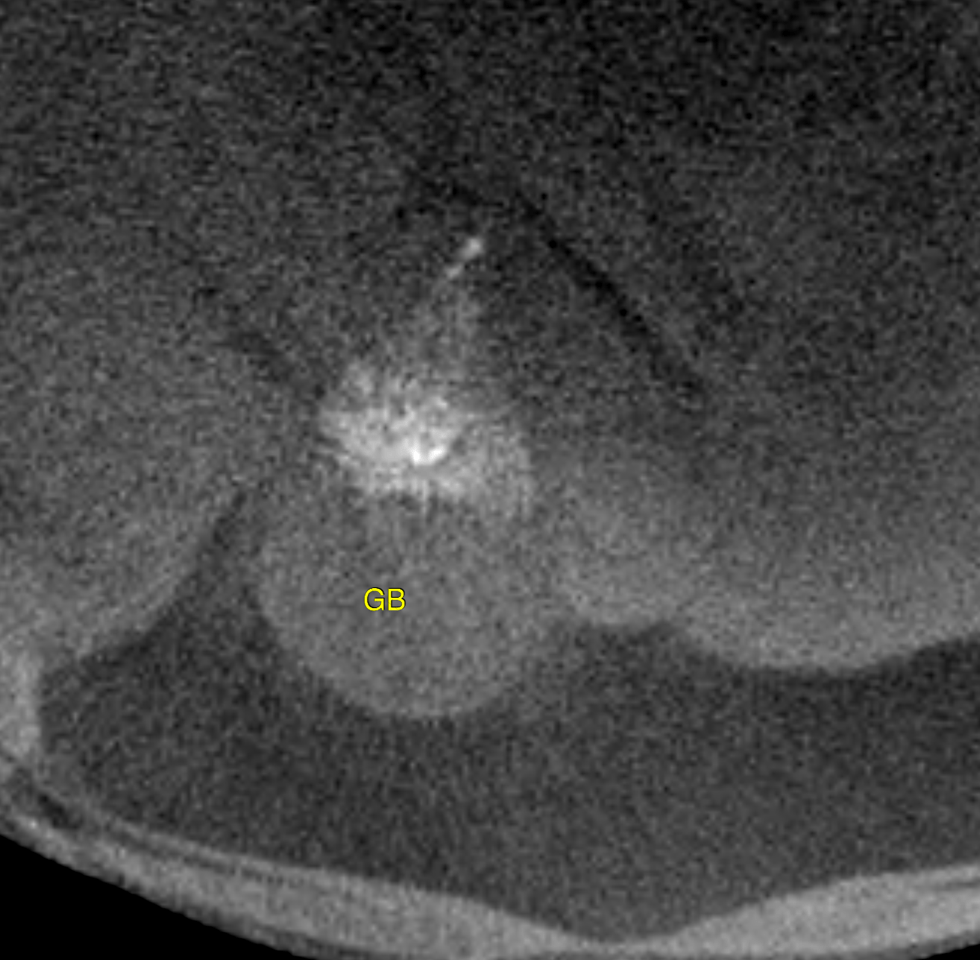
Incidental non-obstructive gallbladder sand/calculi are seen precipitating gravity
dependent within the region of the cystic duct.
Bronchiectasis is an irreversible sequel to long-standing or recurrent
bronchopneumonia, allergic airway disease, smoke inhalation or primary ciliary
dyskinesia (which does not match the age of the dog here).
In general all types of infectious, such as viral, bacterial and less likely fungal or
parasitic, or eosinophilic bronchopneumopathy may be the underlying cause of
bronchiectasis. The lack of bronchial wall changes and pulmonary secretions is unusual though. Note that positive pressure breathhold techniques and endotracheal
intubation as mandatory during the scan but may exacerbate the impression of
bronchial dilation and obscure tracheal and/or bronchial collapse.
The peripheral ground glass opacities within the caudal lung lobes are consistent with
positional atelectasis.
A cardiac disease was not identified as underlying cause of the clinical presentation.
Consider bronchoscopy with bronchoalveolar lavage for further workup to verify the
suspicion of inflammatory/infectious bronchopneumopathy.