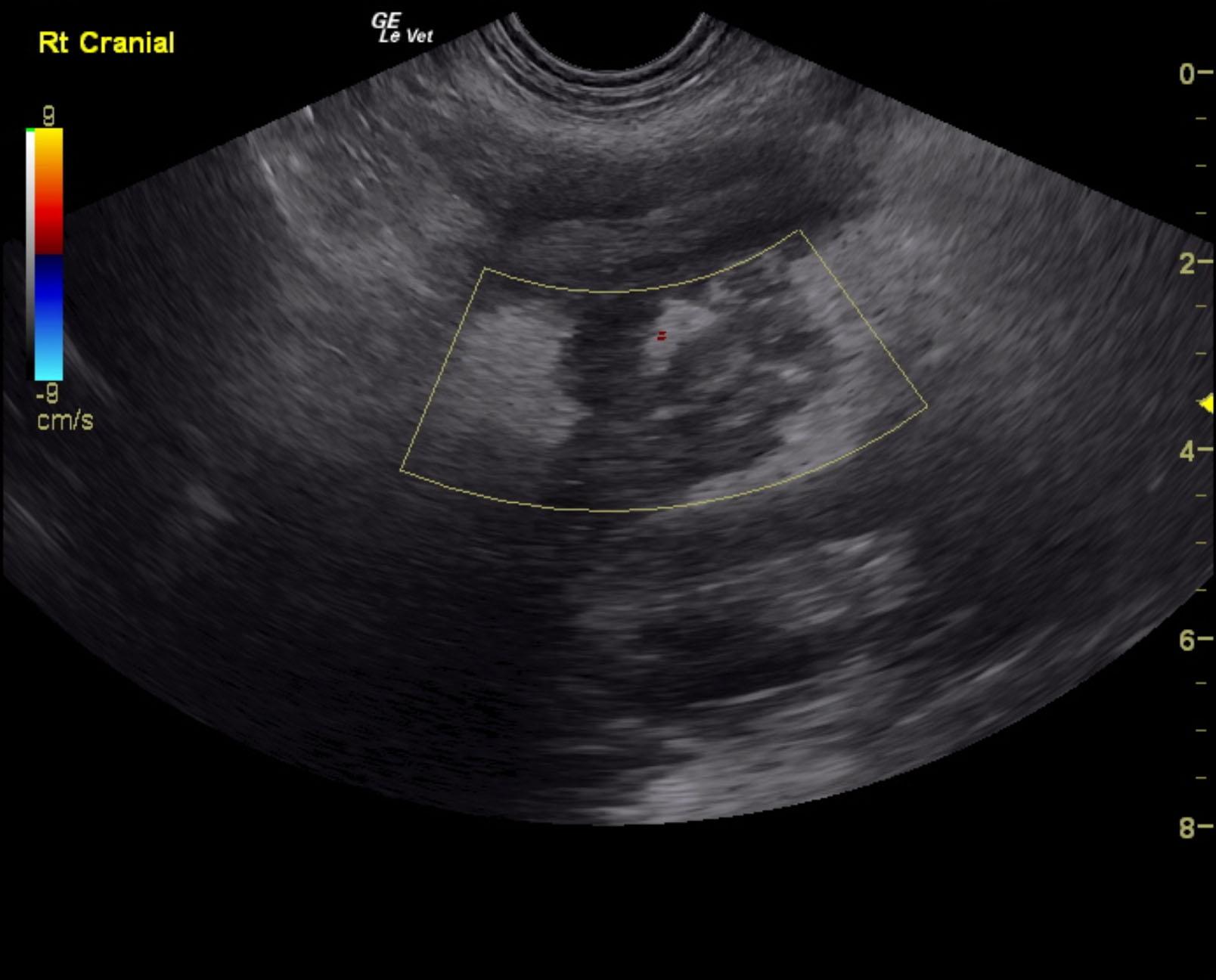
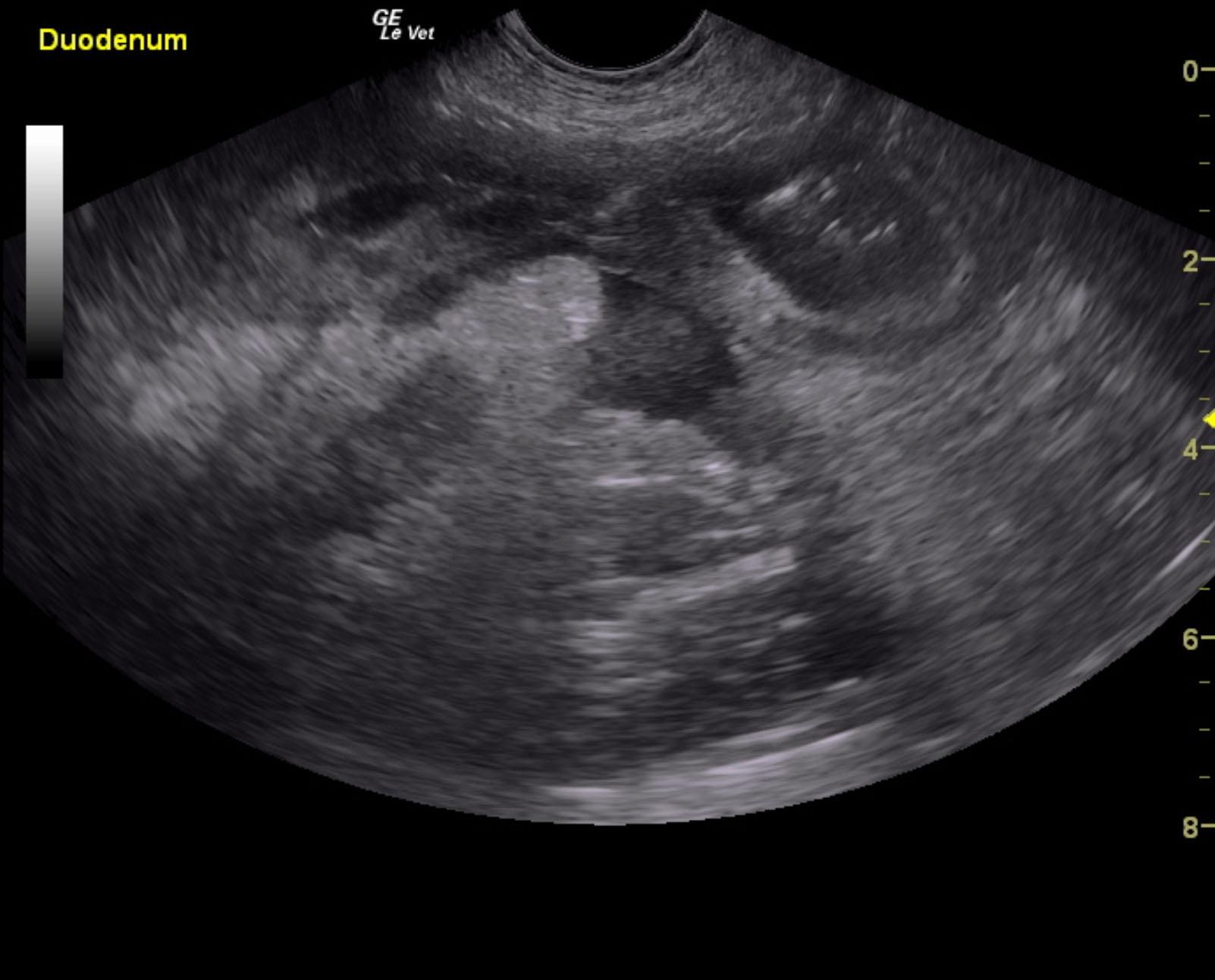
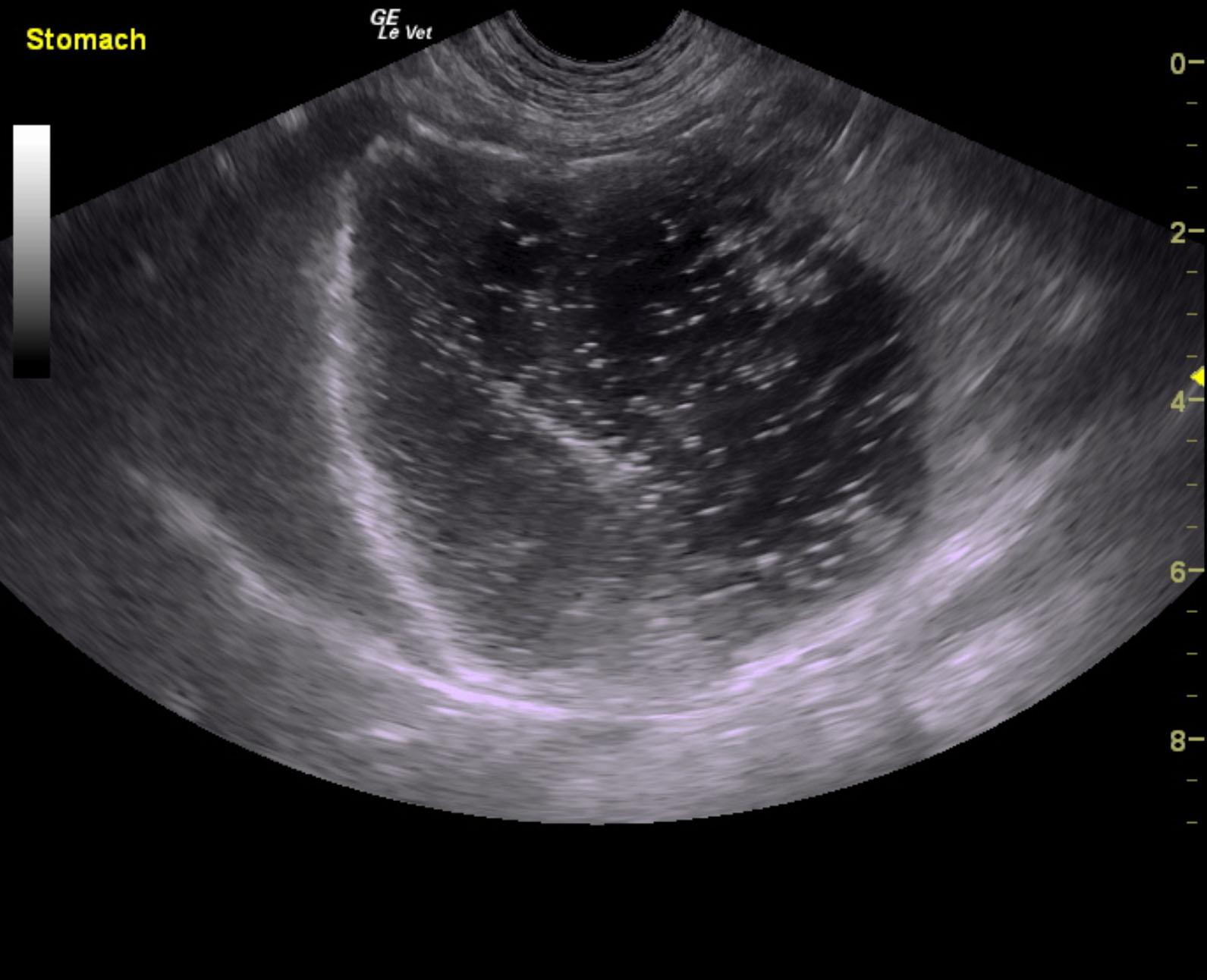
A 4-year-old SF Cockapoo with a history of seizures was presented for evaluation of acute vomiting and pancreatitis. Abnormalities on serum biochemistry were elevated BUN and GGT activity and severely elevated ALP activity and lipase.
A 4-year-old SF Cockapoo with a history of seizures was presented for evaluation of acute vomiting and pancreatitis. Abnormalities on serum biochemistry were elevated BUN and GGT activity and severely elevated ALP activity and lipase.