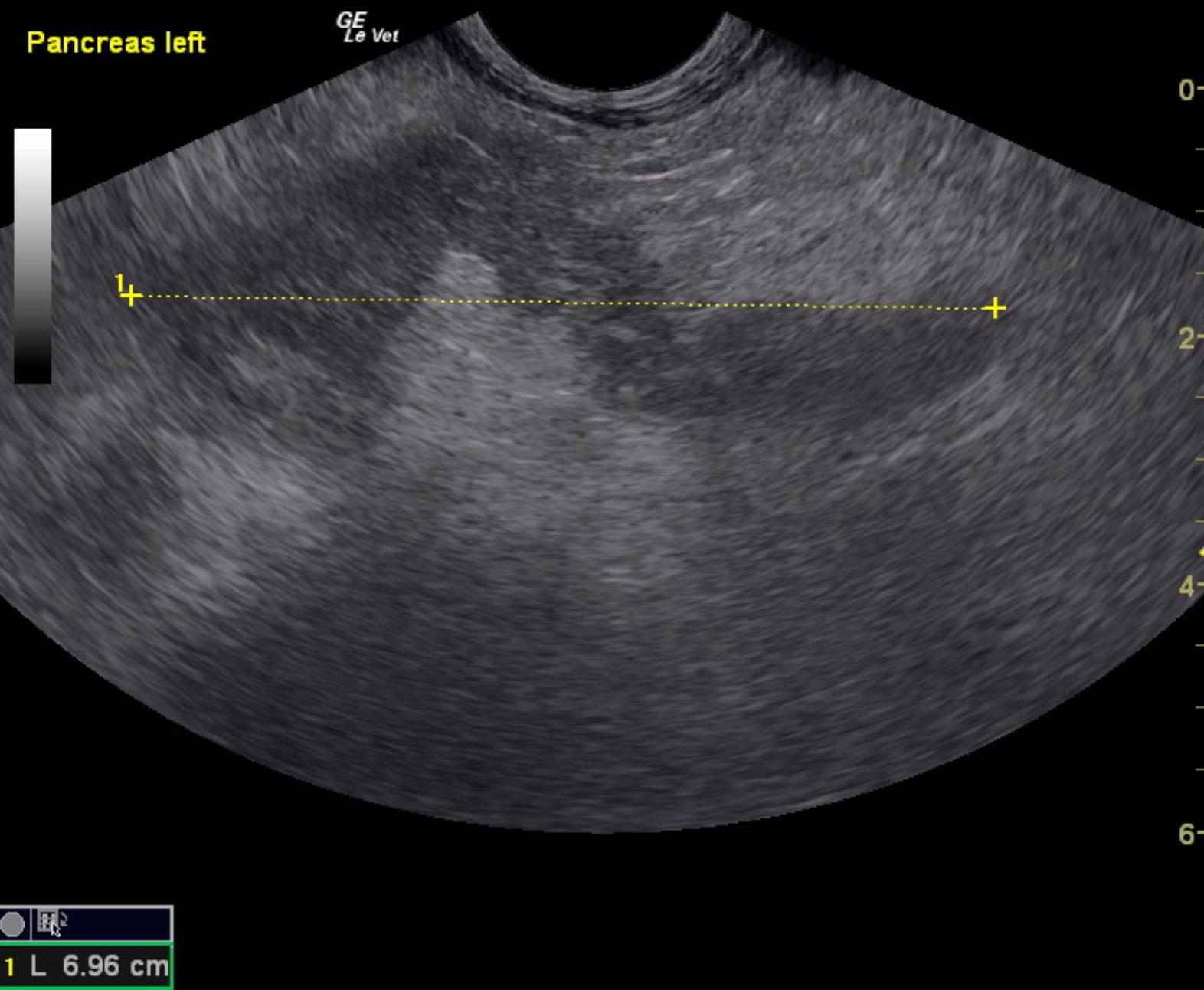
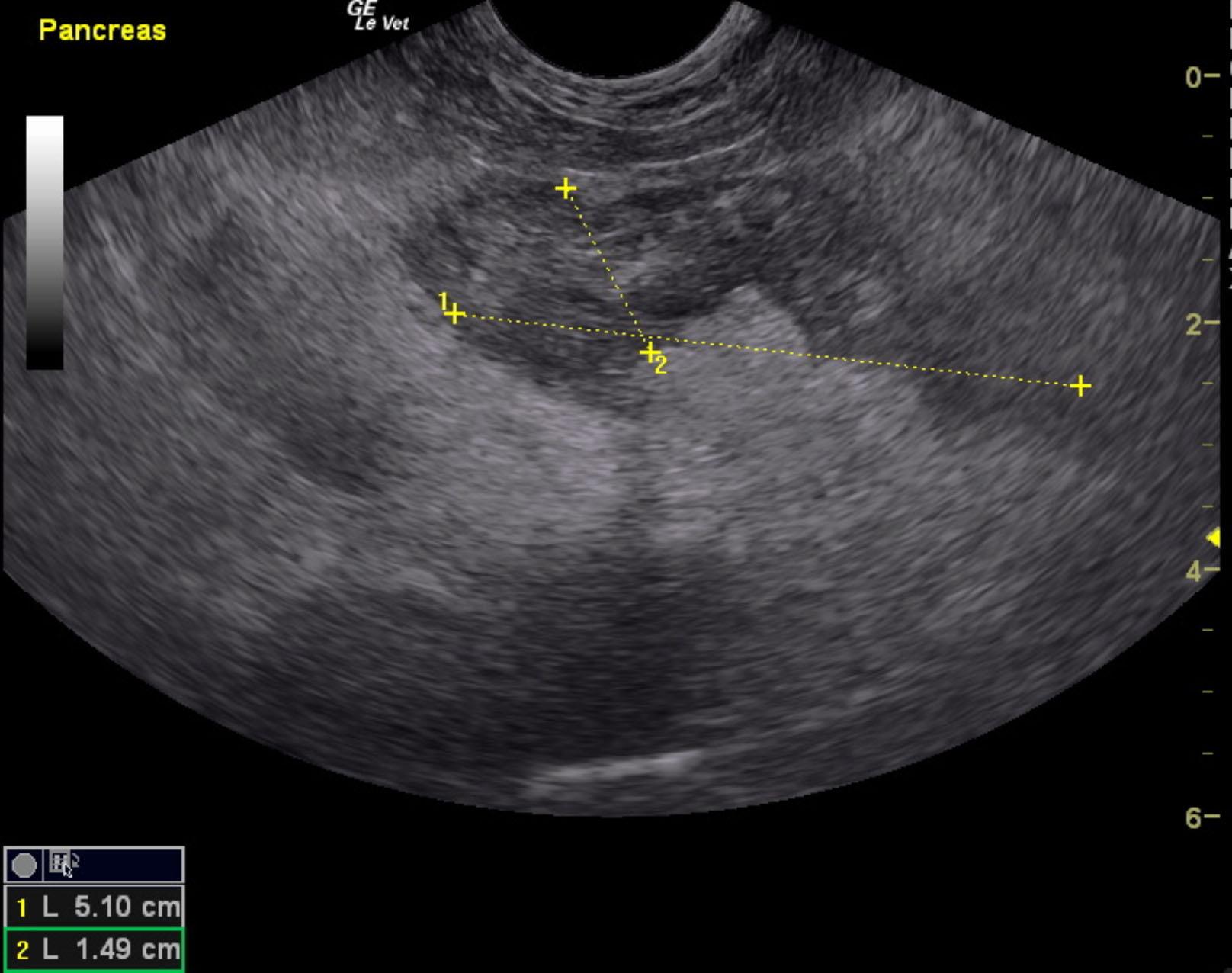
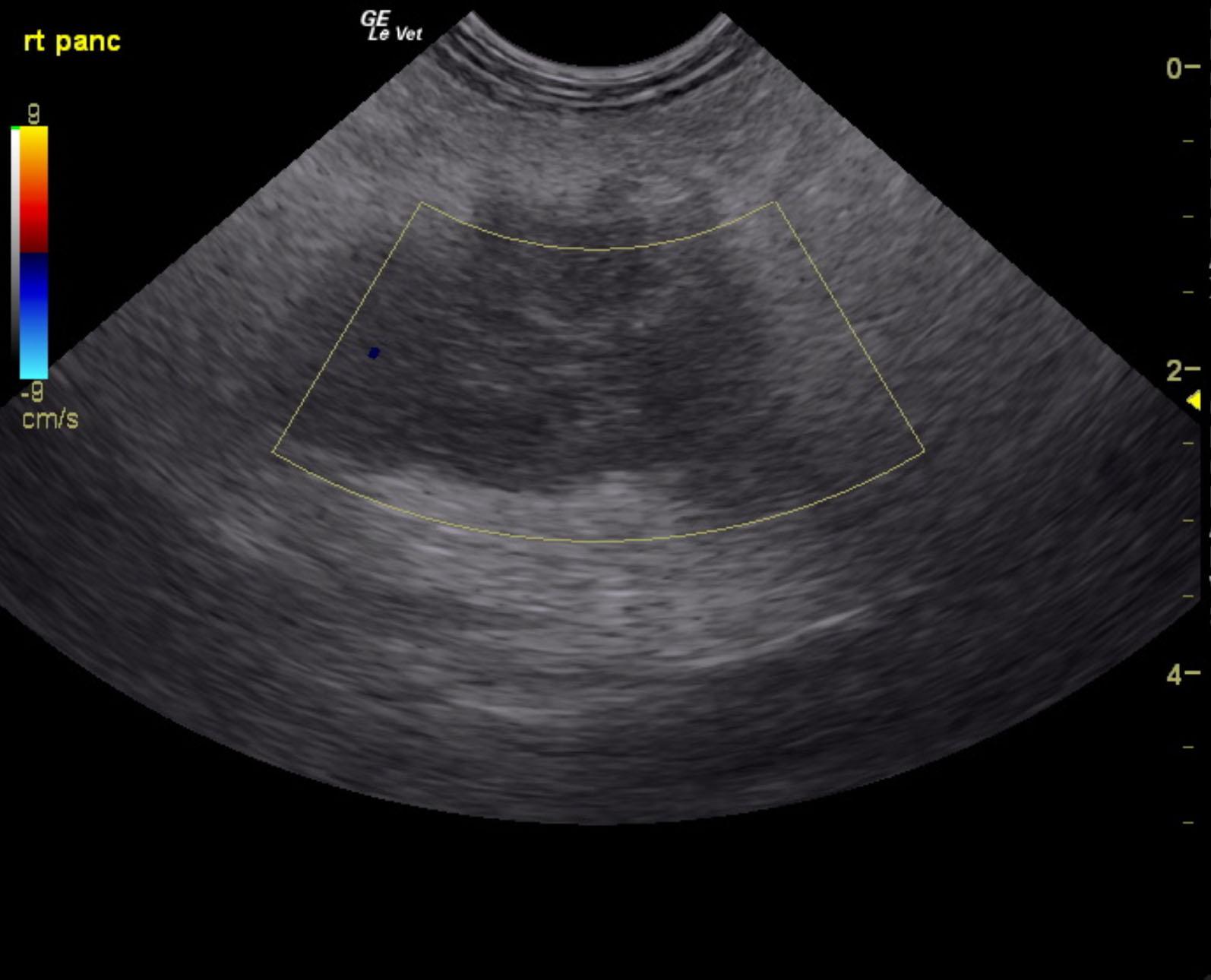
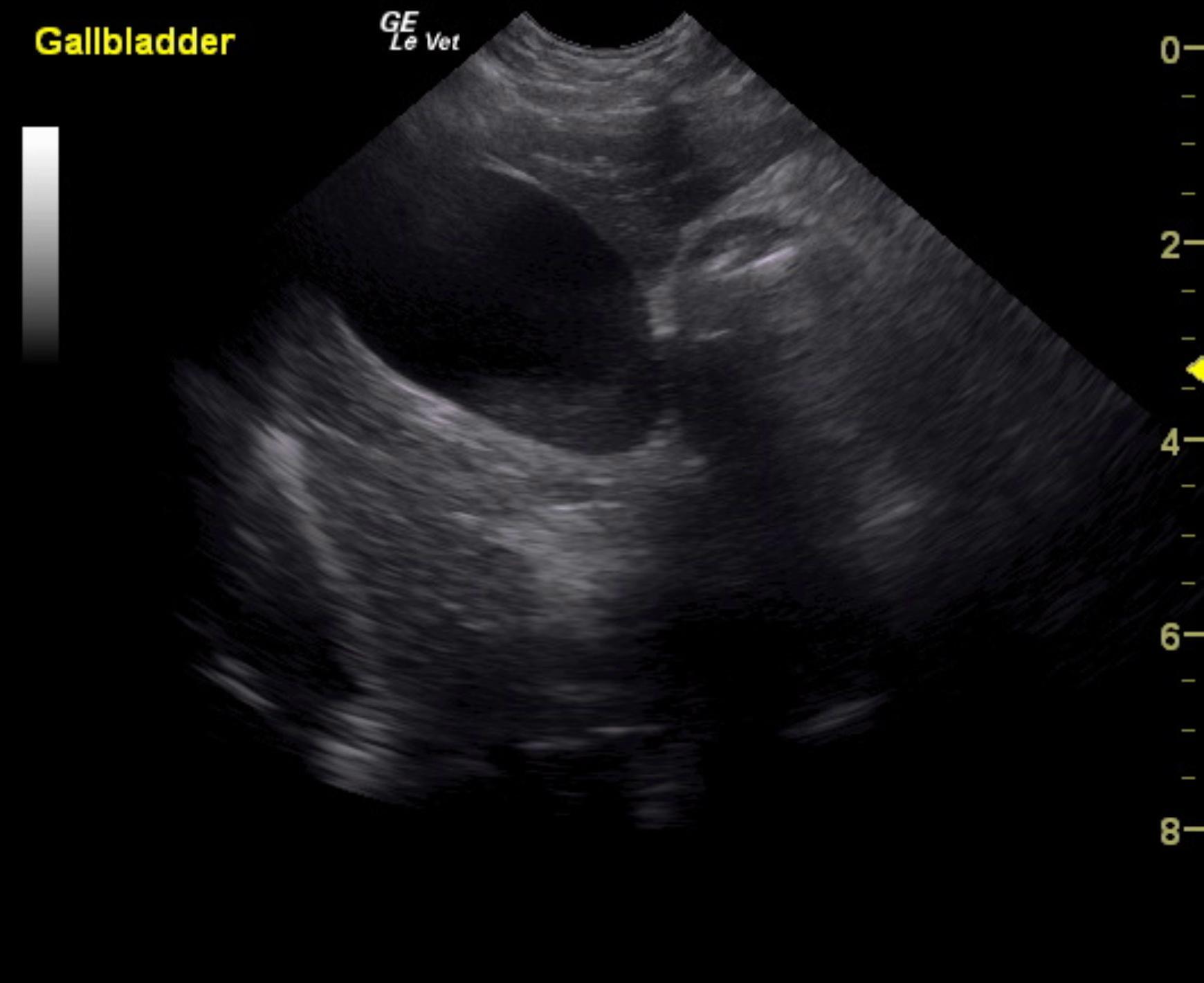
An 11-year-old neutered male Toy Poodle dog was presented for evaluation of protracted vomiting with a history of Addison’s disease (managed with daily prednisone and monthly DOCP injections) and recently diagnosed with diabetes mellitus (managed with insulin). On serum biochemistry, hyperglycemia (288), mildly elevated ALP, and mildly elevated amylase were present.
An 11-year-old neutered male Toy Poodle dog was presented for evaluation of protracted vomiting with a history of Addison’s disease (managed with daily prednisone and monthly DOCP injections) and recently diagnosed with diabetes mellitus (managed with insulin). On serum biochemistry, hyperglycemia (288), mildly elevated ALP, and mildly elevated amylase were present.