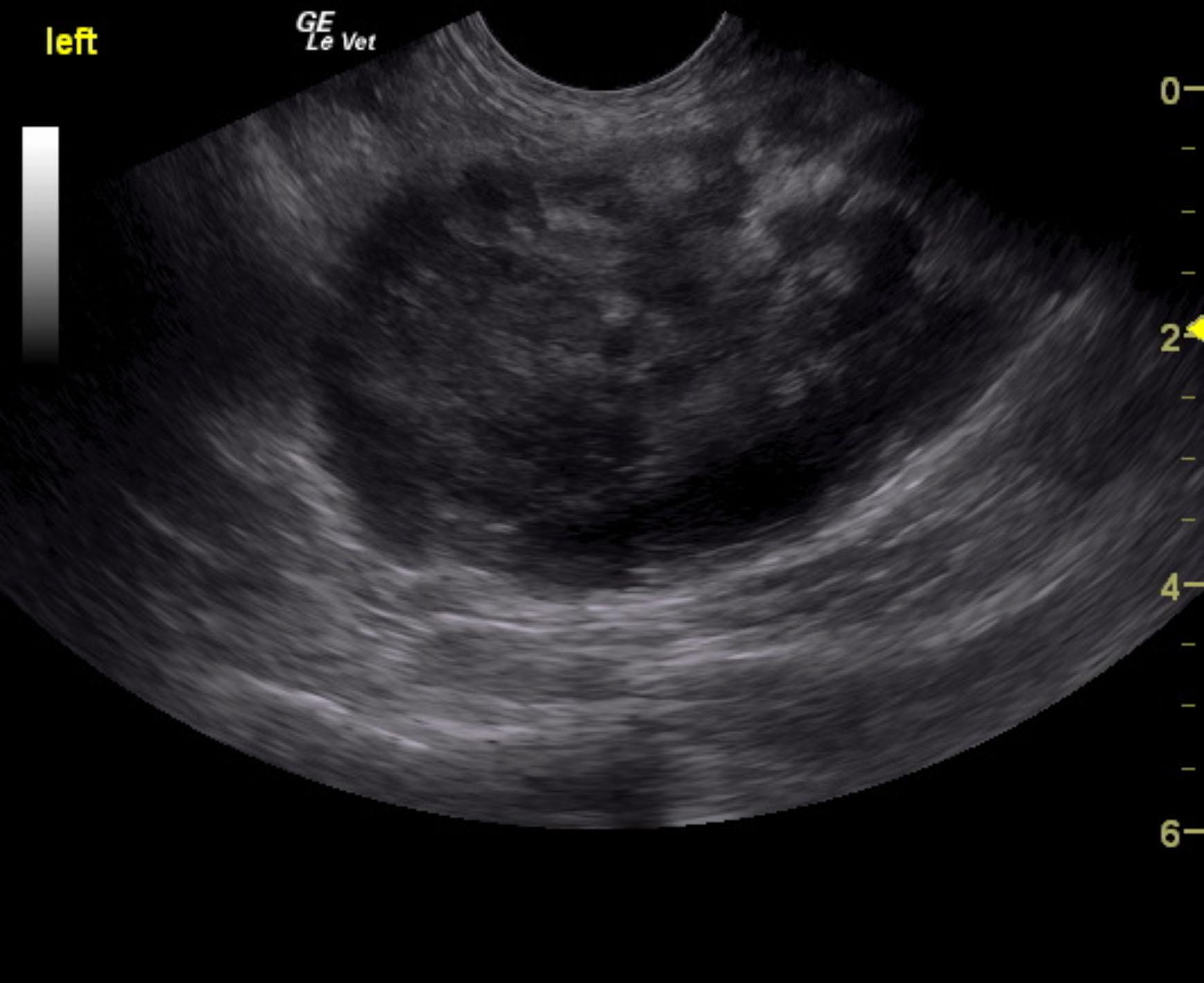
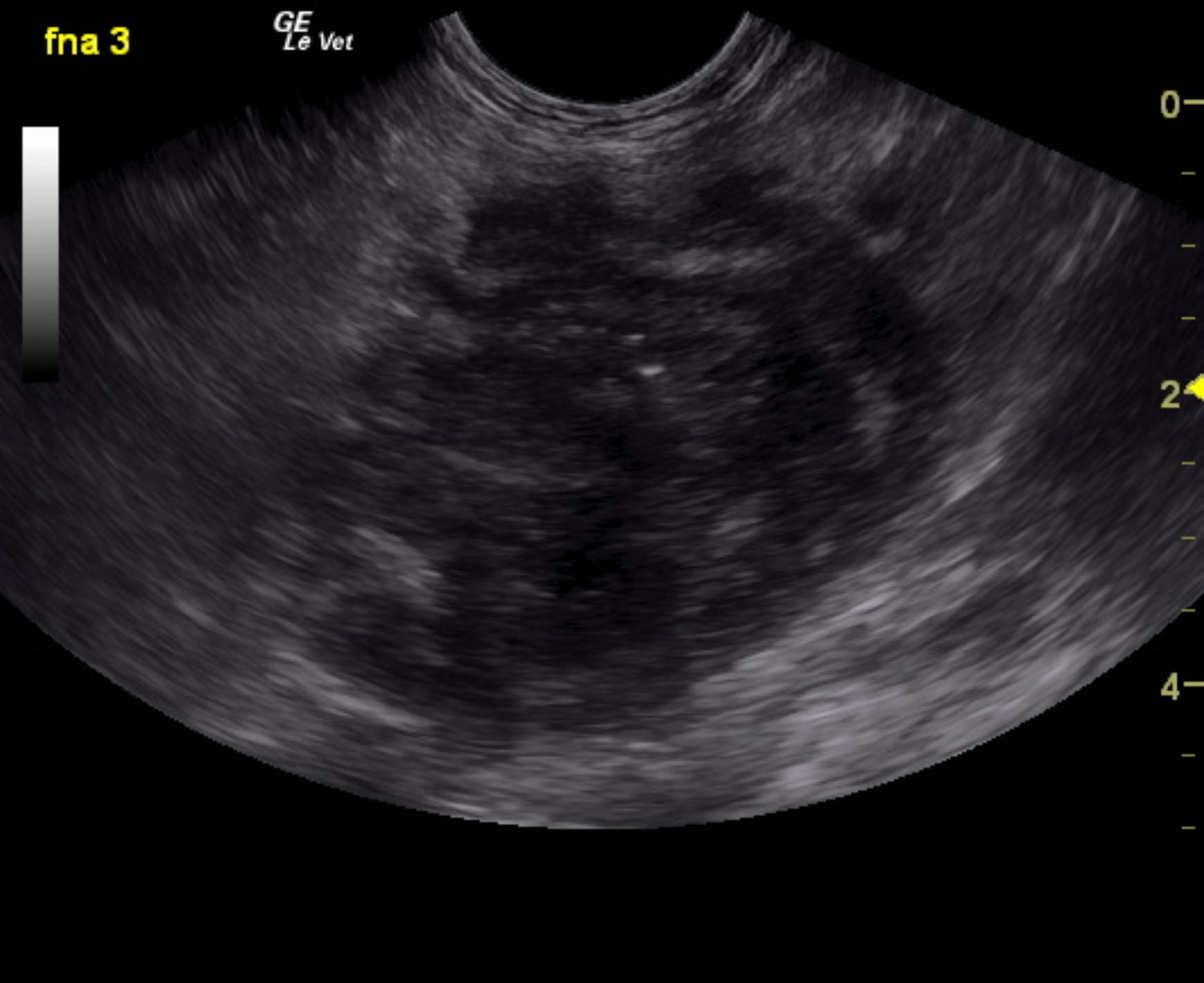
A 16-year-old SF DSH with a history of diabetes and hyperthyroidism was presented for evaluation of vomiting, diarrhea, and anorexia. Urinalysis showed SG of 1.017, proteinuria, and hematuria with negative bacterial growth. Coagulation panel was mildly elevated.
A 16-year-old SF DSH with a history of diabetes and hyperthyroidism was presented for evaluation of vomiting, diarrhea, and anorexia. Urinalysis showed SG of 1.017, proteinuria, and hematuria with negative bacterial growth. Coagulation panel was mildly elevated.