The patient is an 8 year old, FS, canine French bulldog. Clinical exam findings: vomiting, anorexia for 4 days. Possible mass effect. Barium study performed, normal and non-diagnostic.
The patient is an 8 year old, FS, canine French bulldog. Clinical exam findings: vomiting, anorexia for 4 days. Possible mass effect. Barium study performed, normal and non-diagnostic.
Case Study
Jejunal foreign body, 8 Year Old FS French Bulldog
Sonographic Differential Diagnosis
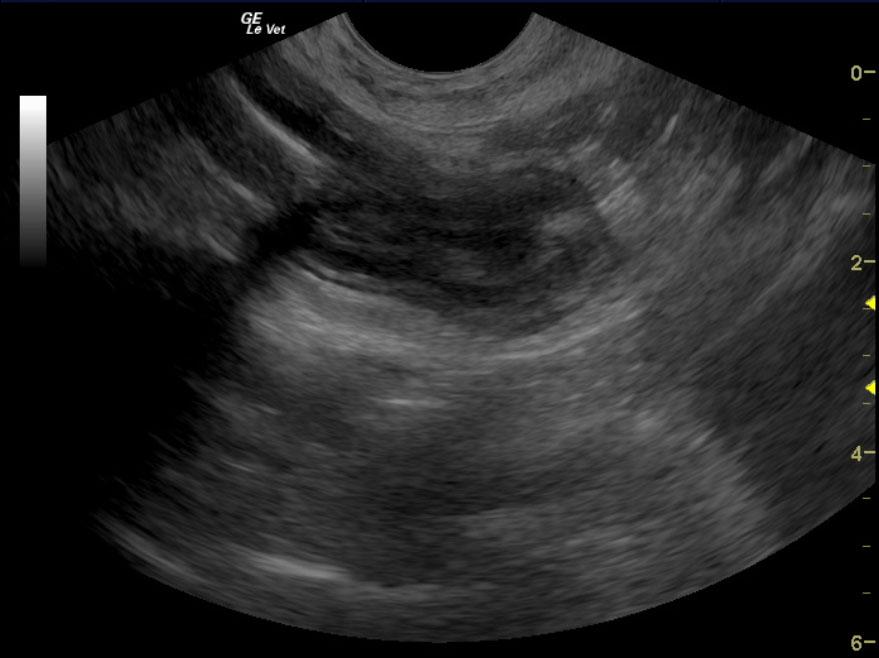
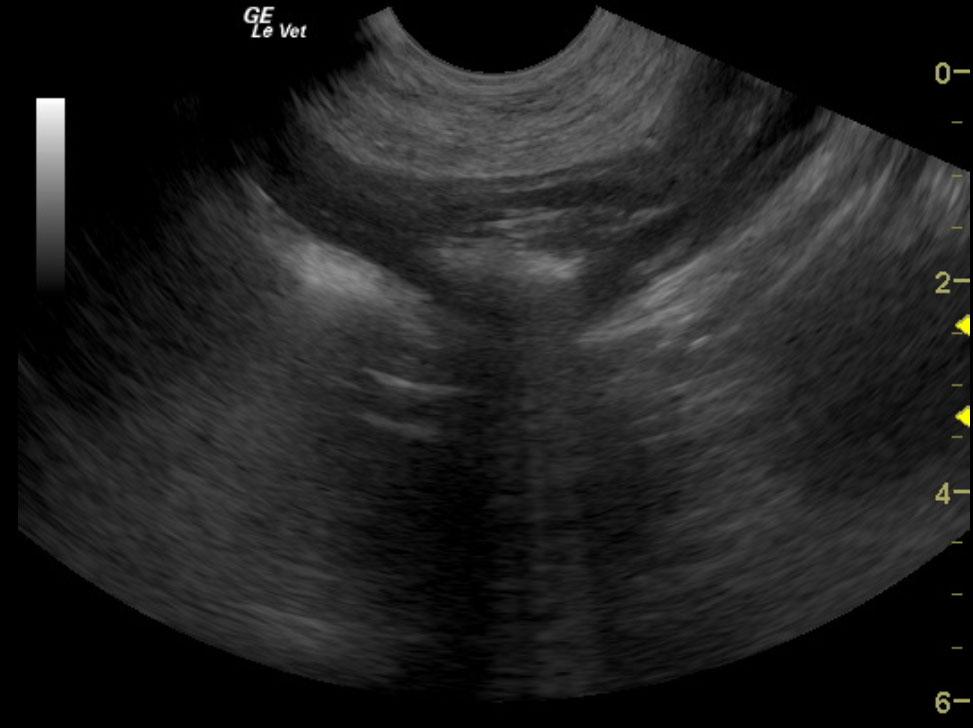
Intestinal foreign body with intestinal perforation and peritonitis. Gas penetration within the wall. Suspect anaerobic component.
Image Interpretation
The gastrointestinal tract revealed variable gastrointestinal wall thickening with foreign body shadowing in the mid small bowel with reactive surrounding fat attached to the omentum. Retained ingesta was also noted and created an obstructive pattern with dilated small intestine followed by empty small intestine. Reactive omentum was noted throughout this region. Some gas penetration was noted in the wall of the intestine, which suggest potential anaerobic component. The stomach appeared empty, yet hypertrophied. Underlying, chronic, mural gastrointestinal disease is likely present. Spontaneous necrosis or multi focal intestinal mural disease is present with secondary foreign body ingestion or possible chronic foreign body ingestion and secondary necrosis. Given the free fluid, reactive omentum, and partial obstructive pattern, immediate exploratory surgery would be recommended with intestinal resection and anastamosis preferably guided by intraoperative ultrasound. The surgeon should be prepared for abdominal lavage. The foreign structure appears to be approximately 1-1.5 inches in length.
DX
Jejunal foreign body, jejunal obstruction
Outcome
Exploratory was performed and a squeaker from a squeaker toy was found.
Clinical Differential Diagnosis
vomiting – IBD, neoplasia, foreign body, non-specific enteritis (viral/bacterial/toxins), dietary hypersensitivity, pancreatitis, pancreatic neoplasia
Sampling
None
Video
Patient Information
Patient Name :
Vanna T
Gender :
Female, Spayed
Species :
Canine
Type of Imaging : Ultrasound
Book :
yes
Status :
Complete
Liz Wuz Here :
Yes
Code :
04_00330
Clinical Signs
- Anorexia
- Vomiting
Exam Finding
- Palpable mass
Images



Clinical Signs
- Anorexia
- Vomiting