A 2-year-old MN DSH was presented for history of a new murmur.
A 2-year-old MN DSH was presented for history of a new murmur.
A 2-year-old MN DSH was presented for history of a new murmur.
A 2-year-old MN DSH was presented for history of a new murmur.
Hypertrophic cardiomyopathy with mitral insufficiency, presently compensated.
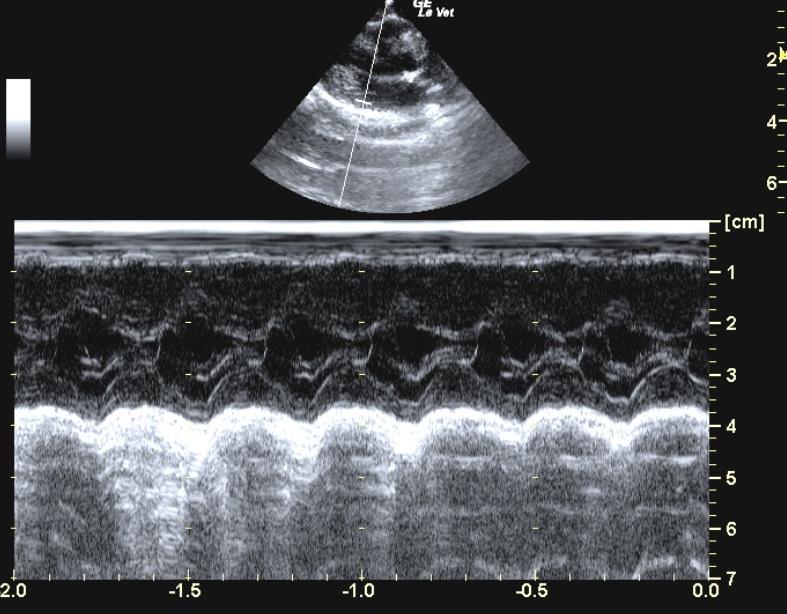
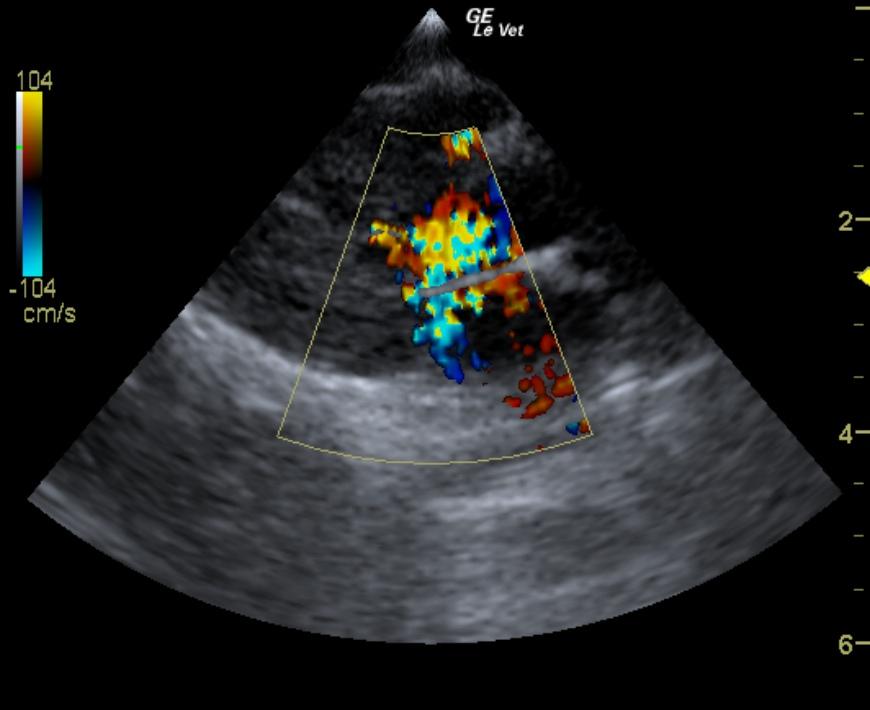
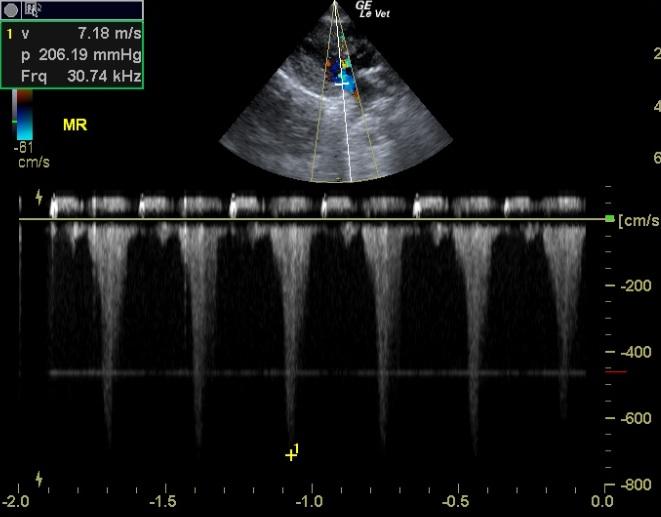
The cranial and caudal mitral valve leaflets demonstrated mildly vegetative contour. Extension and closure were adequate at this time. The left ventricle demonstrated normal volume, but excessive septal and free wall diastolic thicknesses and prominent papillary muscles. This is consistent with either primary hypertrophic cardiomyopathy or secondary hypertrophy (due to systemic disease such as hyperthyroidism or hypertension). Ventricular function was exaggerated consistent with this hyperdynamic state. The aortic outflow tract revealed turbulent flow yet linear valve leaflets with adequate extension, closure and uninterrupted motion. Mitral insufficiency velocity was 7.2 m/sec.
Patient did not return for additional evaluation.
Heart murmur – cardiomyopathy (dilated, hypertrophic, valve insufficiency), physiological (stress, anemia).
If the patient’s resting heart rate was greater than 200 bpm, then Atenolol therapy would be recommended. If not, a recheck echocardiogram in 6 months was advised.