Pre-op castration and hernia repair exam revealed V/VI heart murmur
Pre-op castration and hernia repair exam revealed V/VI heart murmur
Pre-op castration and hernia repair exam revealed V/VI heart murmur
Pre-op castration and hernia repair exam revealed V/VI heart murmur
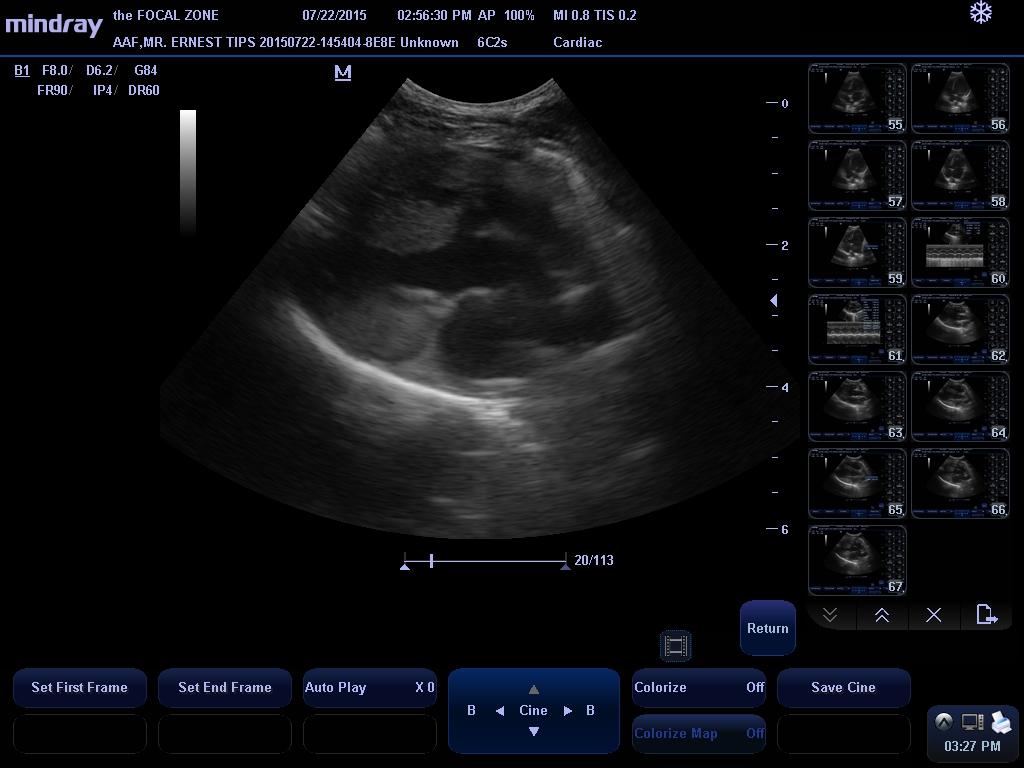
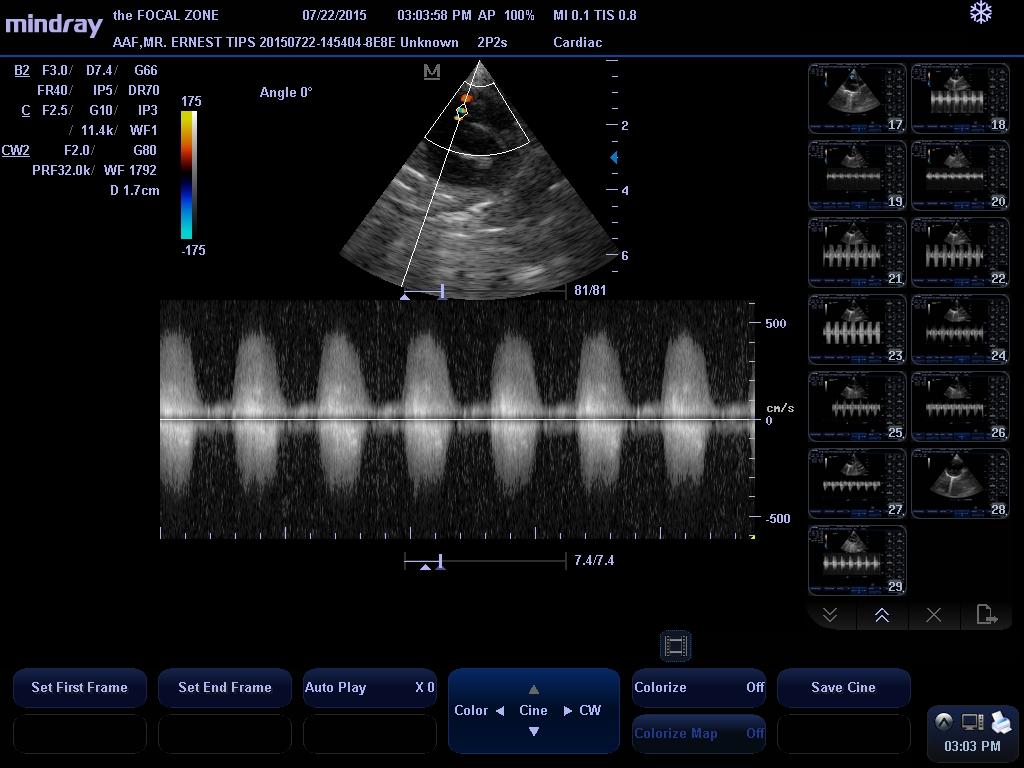
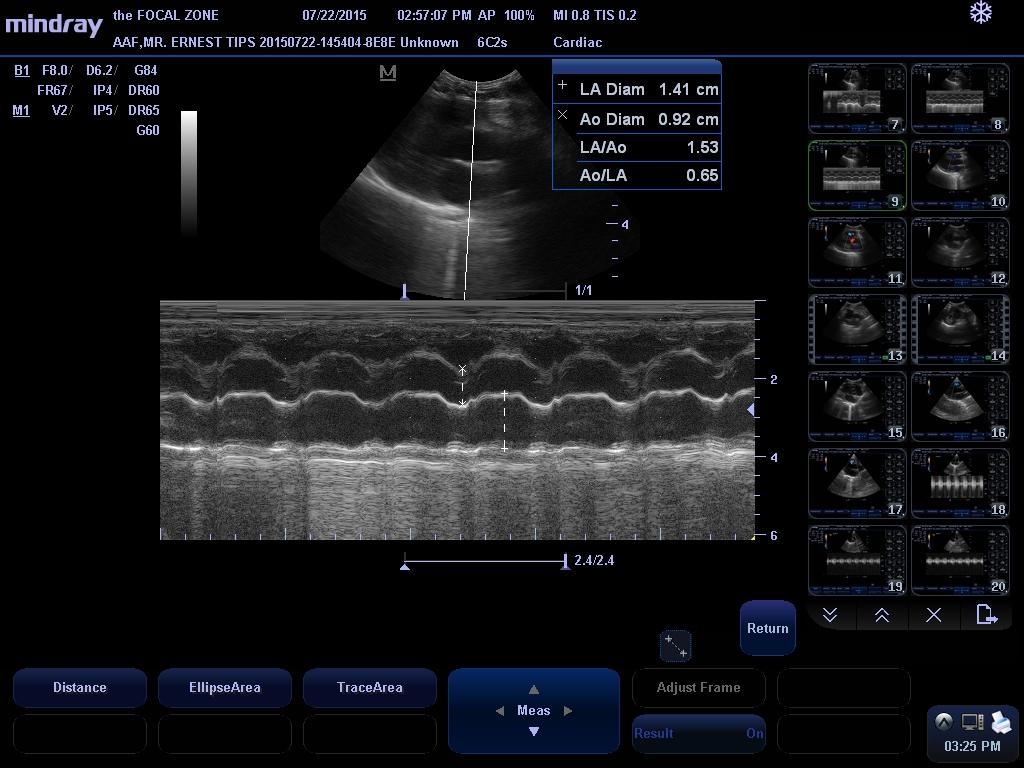
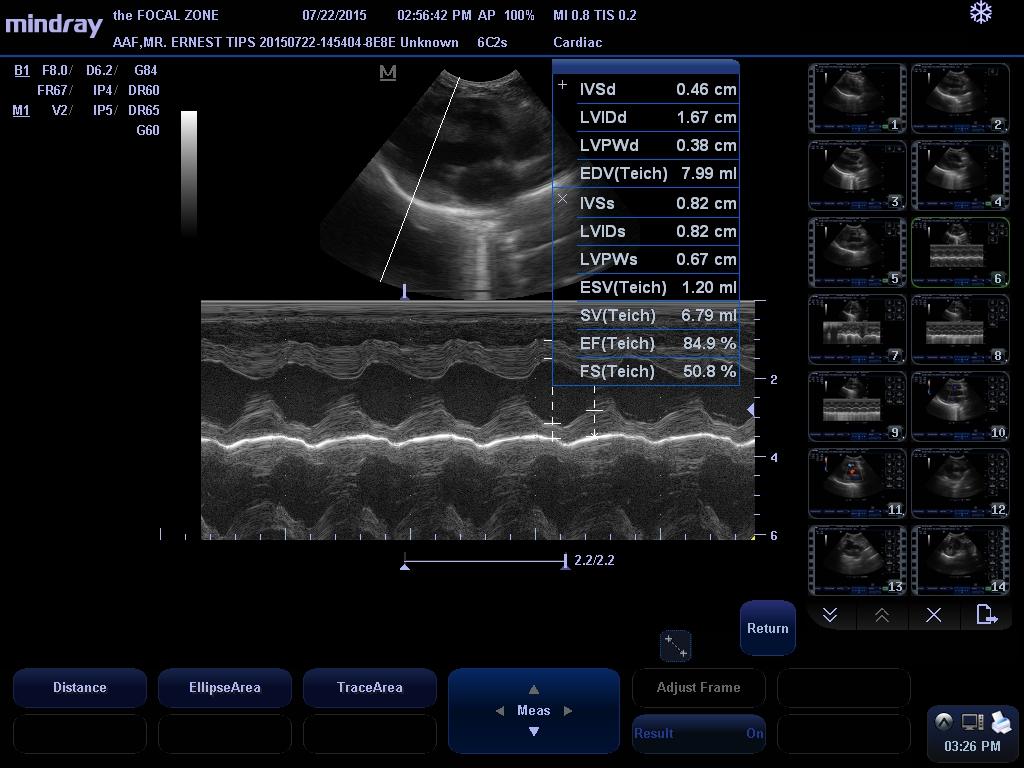
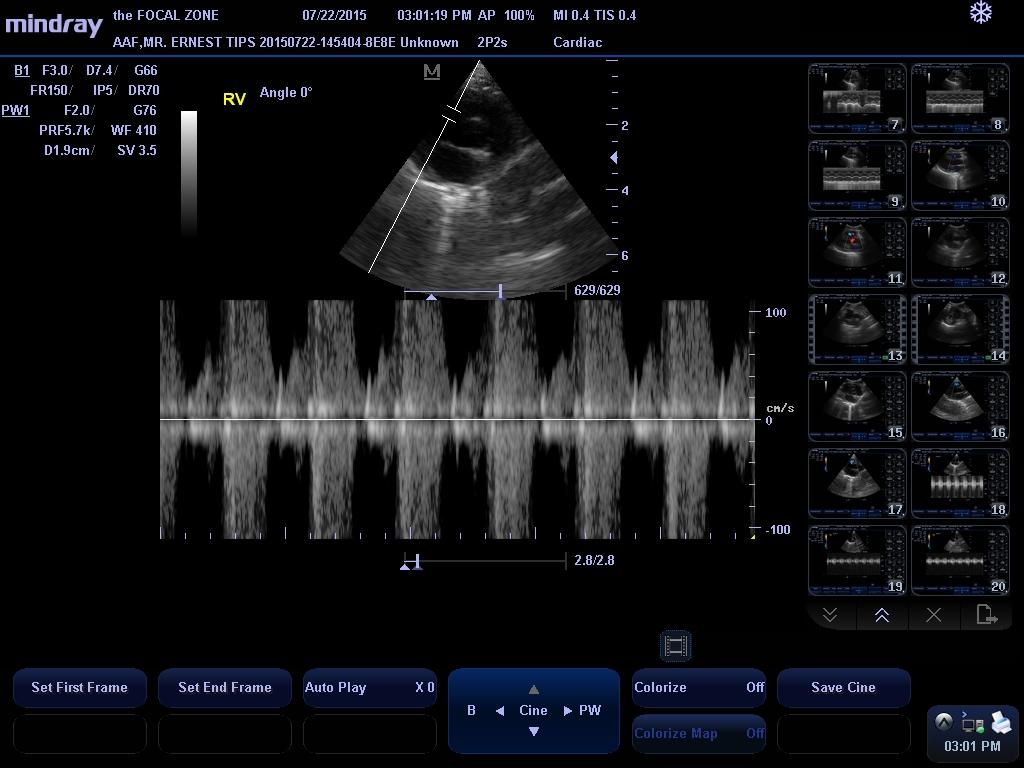
There is mild left atrial and left ventricular dilation. The mitral valve appears normal, though trace physiologic mitral regurgitation is present. Left ventricular wall thickness is normal. Left ventricular systolic function is normal. There is a small perimembranous ventricular septal defect present, with blood shunting from the left atrium into the right atrium. The velocity of shunt flow is consistent with the presence of a restrictive VSD. The aorta and aortic valve are normal. Right atrial and right ventricular dimensions are normal. The tricuspid valve subjectively looks normal, though mild tricuspid regurgitation is present. The pulmonary artery and pulmonic valve are normal. No pericardial effusion or cardiac masses are seen.
LA/Ao – 1.53
IVSd – 4.6 mm
LVIDd – 16.7 mm
LVPWd – 3.8 mm
LVIDs – 8.2 mm
FS – 50.8%
EF – 84.9%
LVOT Vmax – 0.80 m/s
RVOT Vmax – 0.70 m/s
VSD Vmax – 4.9 m/s
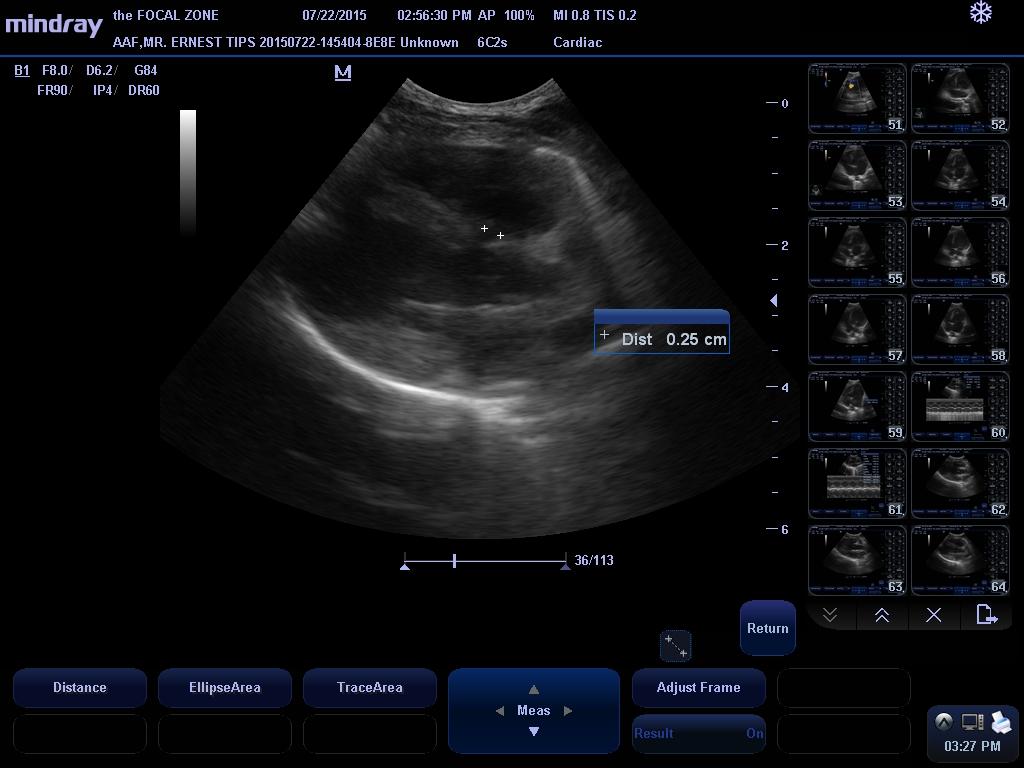
VSD diam – 2.5 mm
Electrocardiogram Findings:
A single lead ECG is submitted for review.
HR: 166 bpm
Rhythm: Sinus
Normal sinus rhythm is present throughout this recording. All complex amplitudes and intervals are within normal limits.
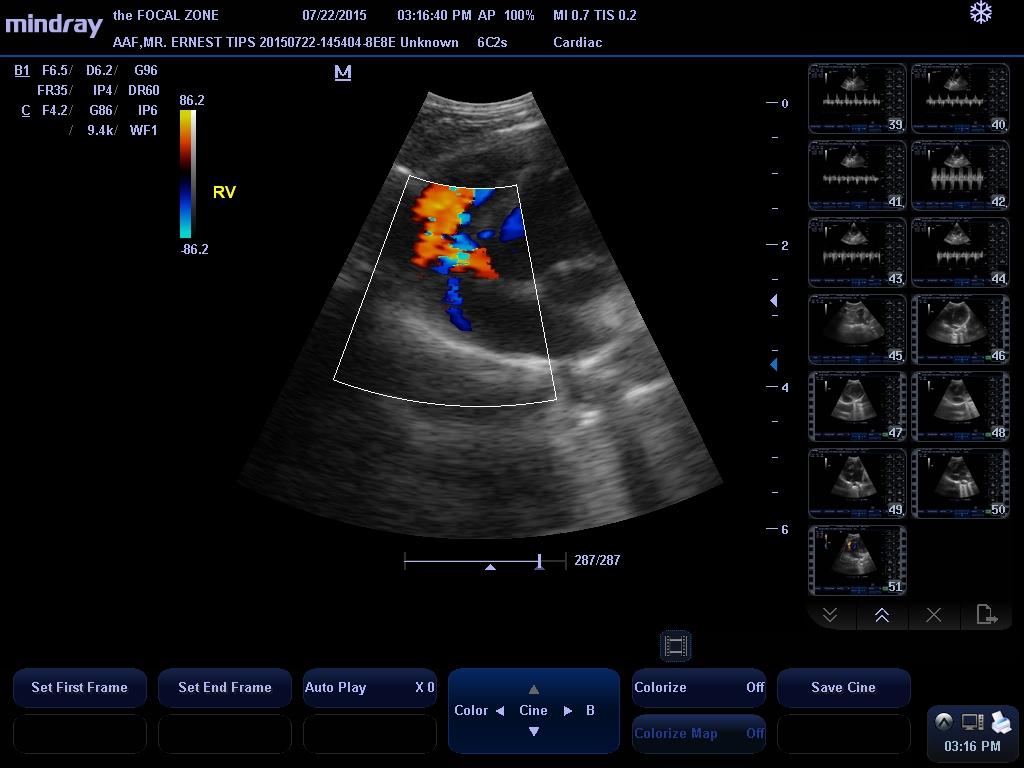
This examination demonstrates a small left to right shunting perimembranous ventricular septal defect with very mild left heart volume overload. The clinical significance of VSDs are dependent on the size of the defect and resistance to flow, which is related to the left and right ventricular systolic pressures. With small defects, there is a high resistance to systolic flow, and thus, there is only a small amount of blood that shunts through the defect, whereas with larger defects, there is a significant amount of shunting that can eventually lead to left-sided congestive heart failure and even shunt reversal if secondary pulmonary hypertension develops. This patient’s VSD appears to be small, and more importantly, his shunt velocity is consistent with a restrictive defect, indicating that the small size of the detect provides high resistance to flow, so that while his murmur is very loud, there is actually only a small volume of blood shunting from the left ventricle to the right ventricle (the loud murmur is caused by the blood squeezing through a small opening). Given the presence of a restrictive defect, it is possible that the VSD may never become clinically relevant, though the presence of mild left heart dilation suggests that his disease must be monitored carefully over time.
This examination also demonstrates mild tricuspid regurgitation, which may be consistent with mild tricuspid valve dysplasia.
The risk for general anesthesia appears to be mildly increased based on this exam, though there does not appear to be an absolute contraindication to general anesthesia.
RECOMMENDATIONS: No therapy appears to be warranted at this time, as the VSD is small and there is minimal left heart volume overload. Should more significant left heart dilation develop, an arterial dilator such as amlodipine and/or enalapril can be given in order to decrease systemic vascular resistance, and therefore, the amount of left to right shunting.
As for general anesthesia, I recommend avoiding the use of alpha-2 agonists, ketamine, and telazol in the anesthetic protocol. Premedication with an opioid/benzodiazepine combination and induction with propofol is recommended.
A recheck is recommended in 6 months to monitor for disease progression.