CT of the abdomen, plain and 2 post-contrast series: The scan did not cover for the region caudal to the renal arteries and veins.
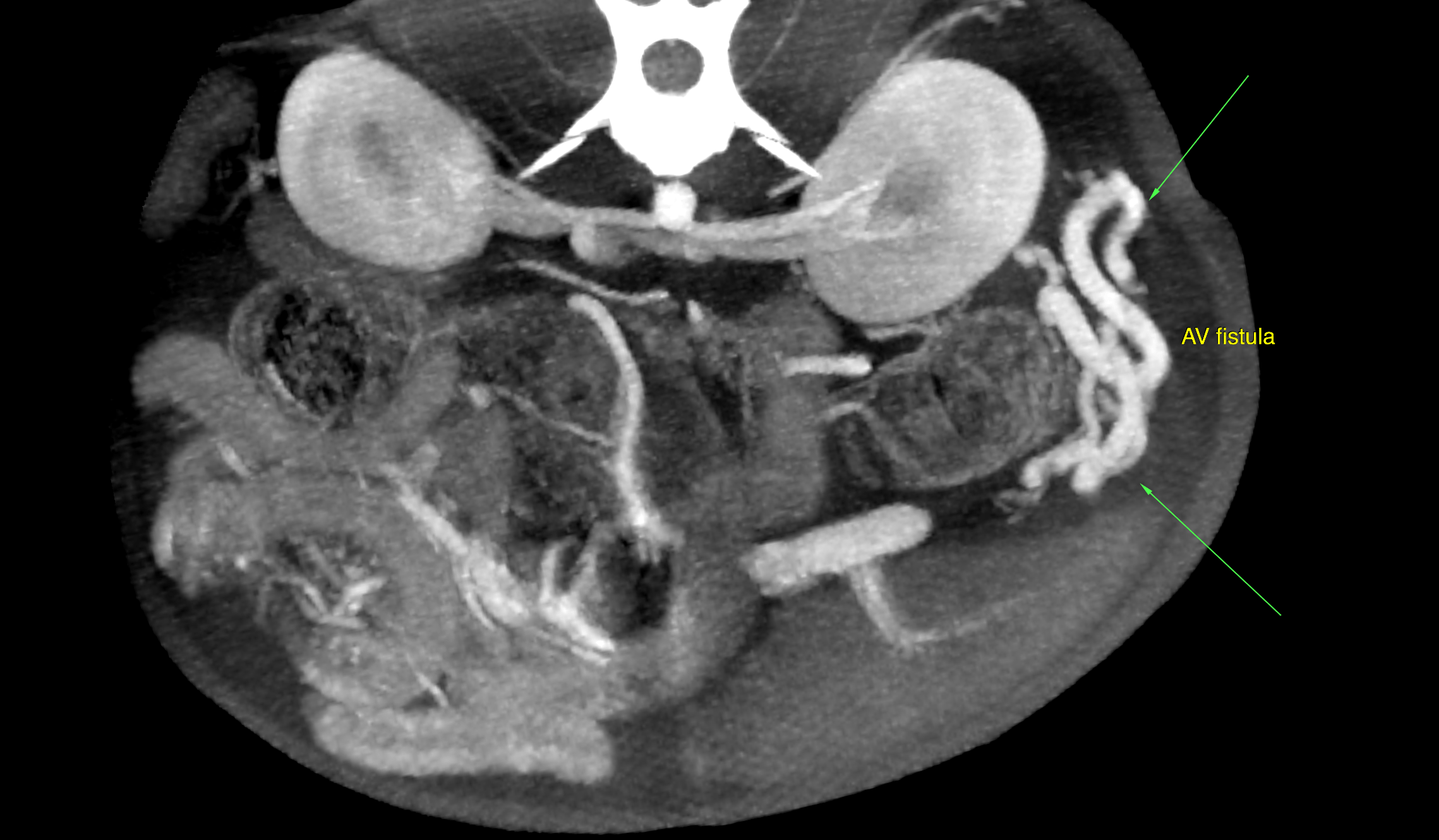
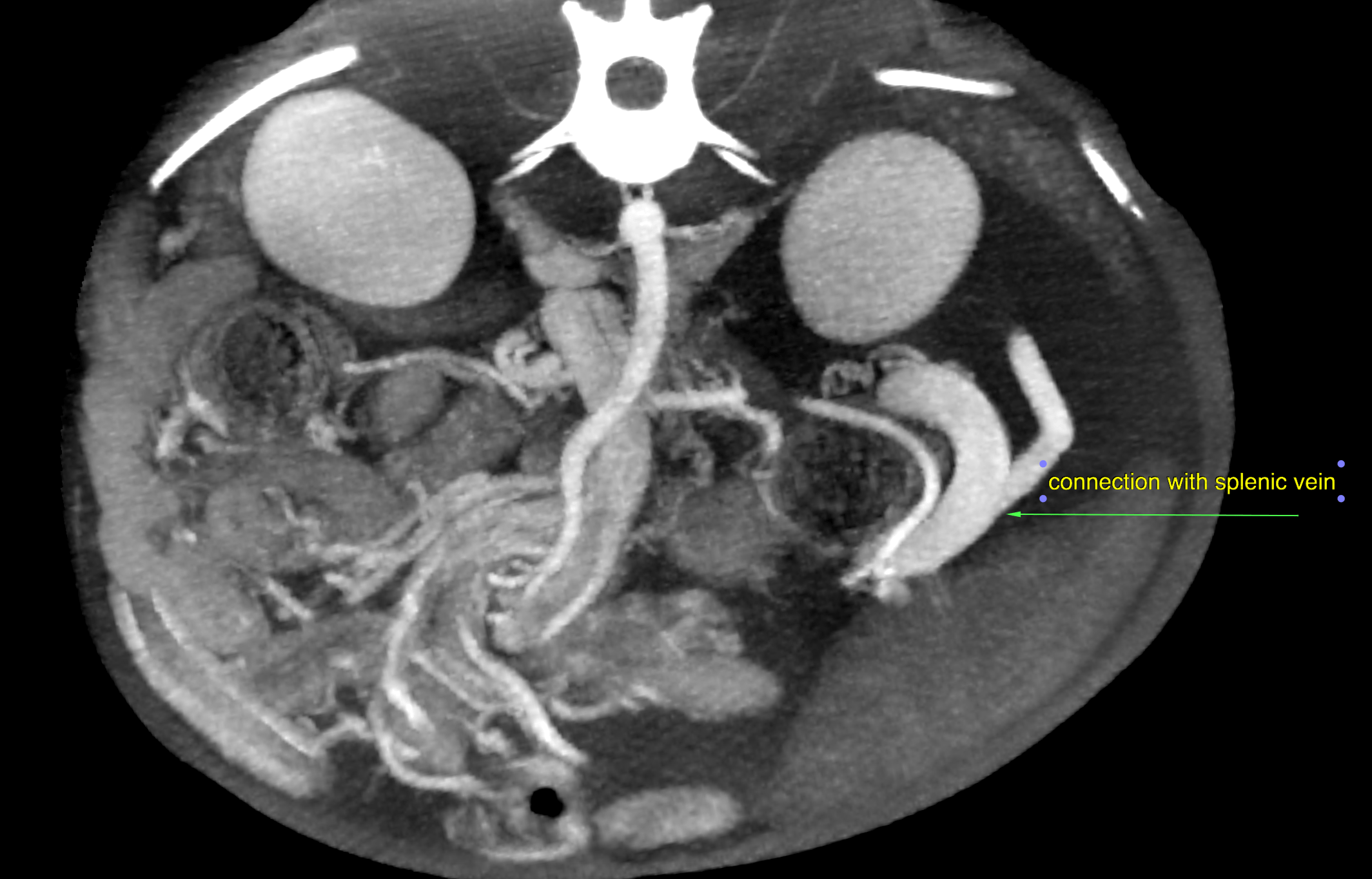
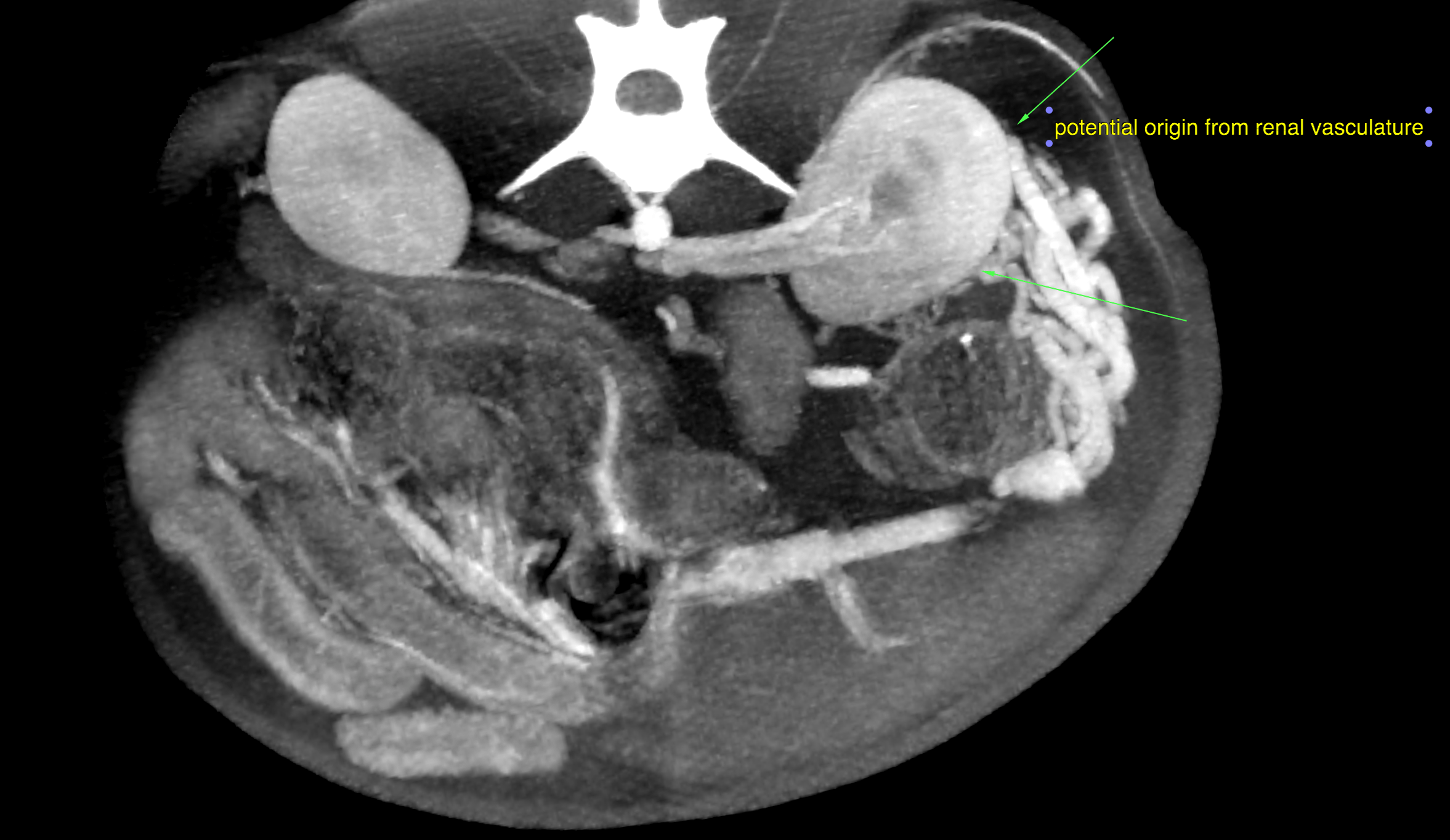
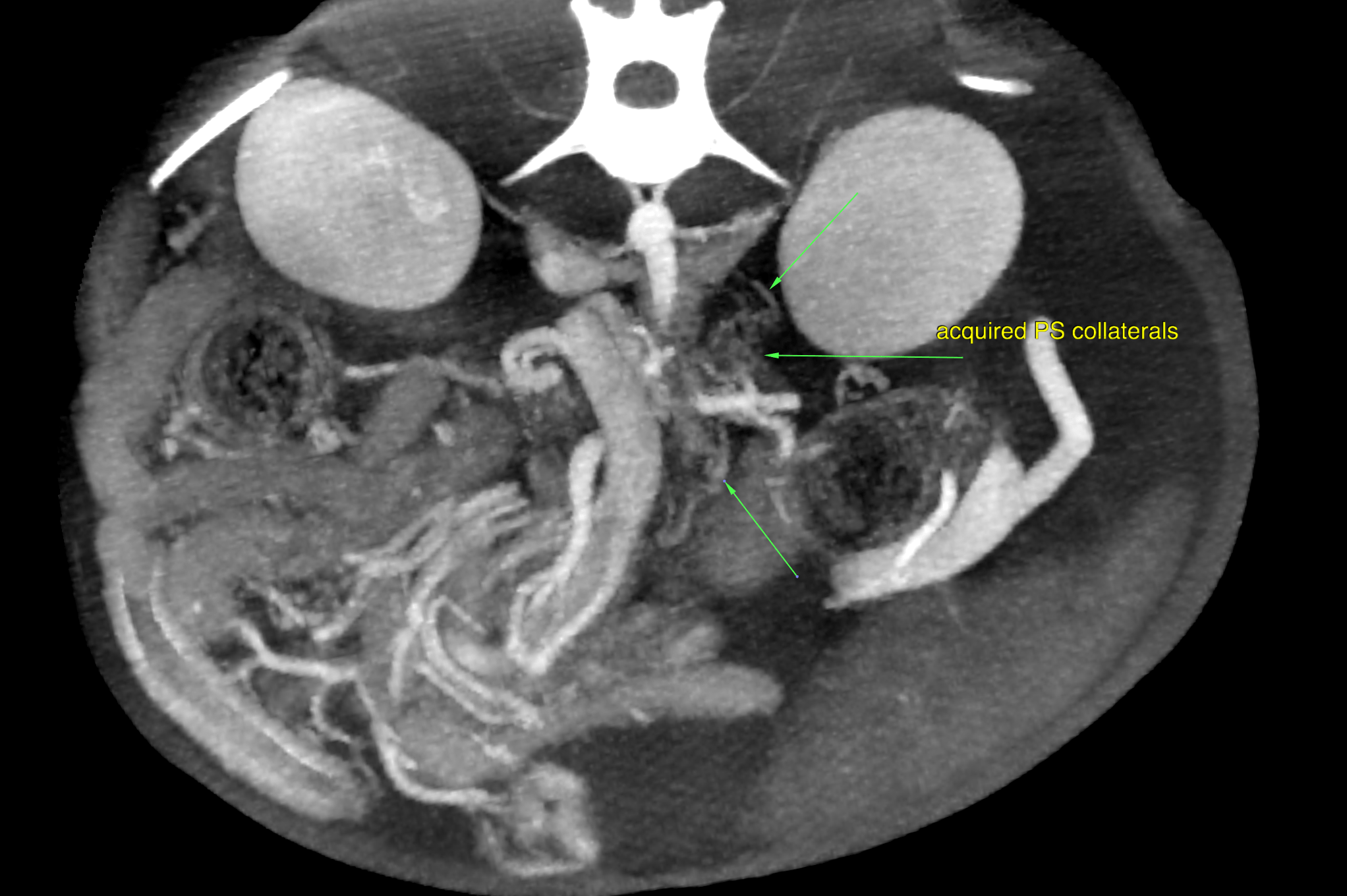
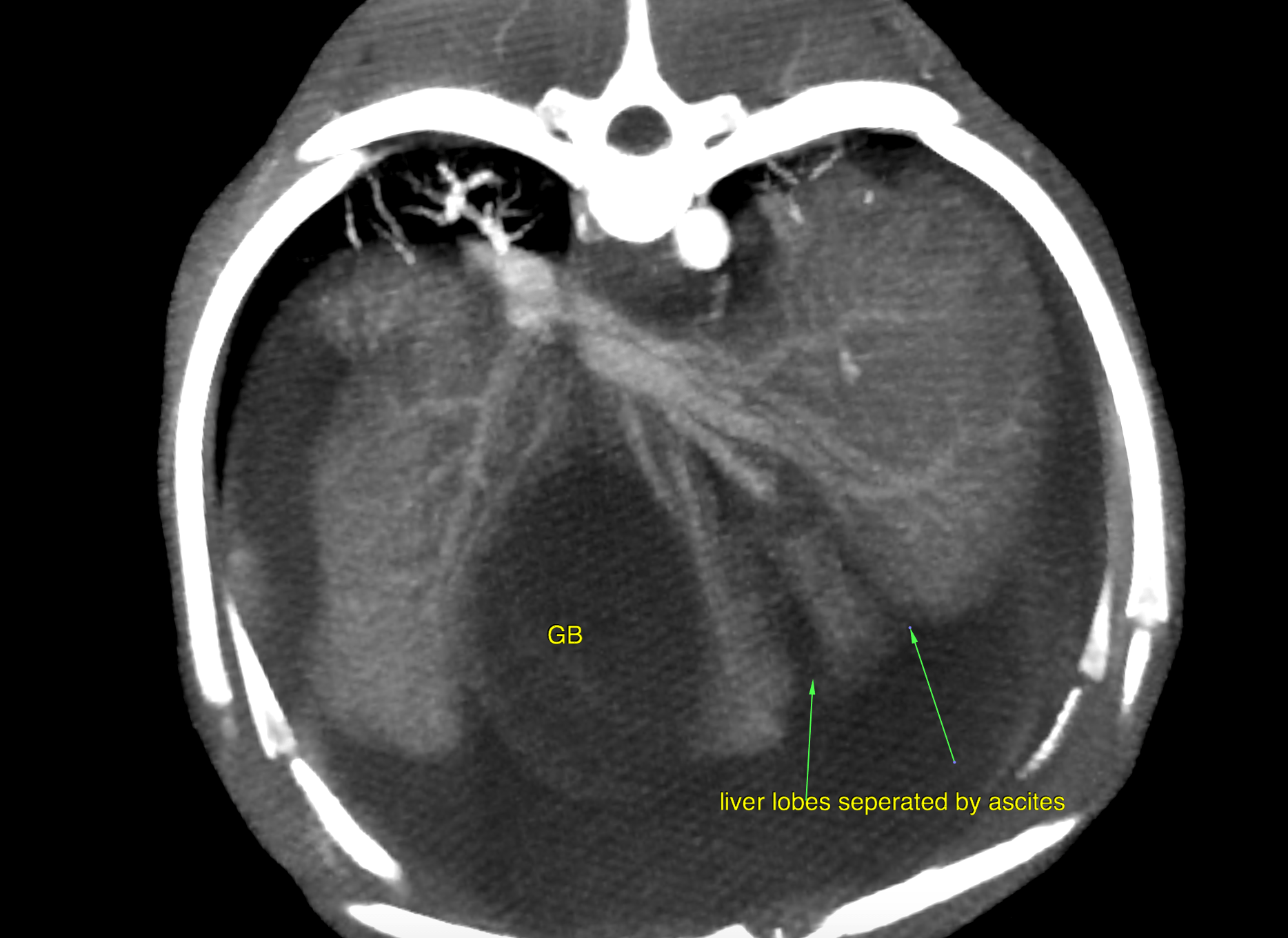
A moderate amount of free peritoneal fluid was present. Microhepatica was noted. The gallbladder was severely distended, and the gallbladder wall was mildly thickened. The spleen was enlarged which was likely a function of congestion. There was multifocal post contrast heterogeneity due to differential enhancement of the red and white pulpa. A single abnormal vessel connecting the portal vasculature with the systemic circulation was not seen. The extrahepatic portal vein was tortuous in course, low for enhancement and uneven in diameter. There was a formation of highly enhancing and tortuously spiraling vessels lateral to the left kidney. The high contrast enhancement was similar to the paralleling arterial enhancement of the aorta, celiac artery and cranial mesenteric artery which may be suggestive for arterial origin here. The caudal vena cava, splenic, and portal vein were lower in enhancement. The described vascular formation connected with the splenic vein on one end. The other end appeared to be connected with small tortuous vessels arising from the left renal cortex. Note that the exact origin of the vascular malformation cannot be defined based on this scan! There also was a formation of thin tortuous vessels in the region between the kidneys consistent with multiple acquired portosystemic collaterals. The intrahepatic branching of the portal vein was within normal limits. The splenic vein was larger in diameter and presented higher contrast enhancement compared to the portal vein. The intraabdominal caudal vena cava was relatively thin compared with the splenic and portal veins.