This 7 year old MN American Bulldog presented with progressive left front lameness. No pain on palpation.
This 7 year old MN American Bulldog presented with progressive left front lameness. No pain on palpation.
This 7 year old MN American Bulldog presented with progressive left front lameness. No pain on palpation.
This 7 year old MN American Bulldog presented with progressive left front lameness. No pain on palpation.
Rads of the right and left elbow, left shoulder and cervical spine –
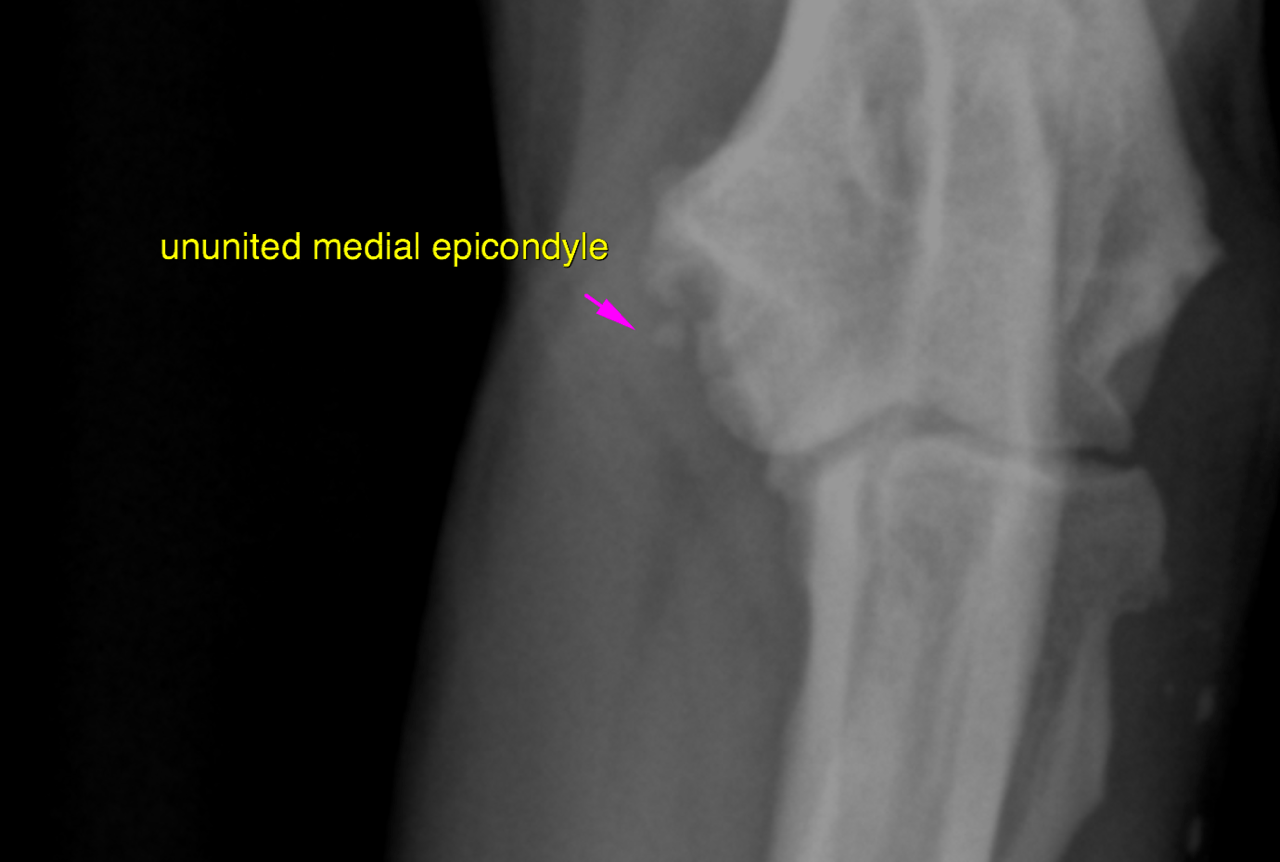
LEFT ELBOW: The cranial contour of the medial coronoid process (MCP) is blurred. Marked loss ofopacity is noted in the proximal aspect oft he MCP. A mild radioulnar step formation with a longer ulna is noted and associated with slight narrowing of the medial joint compartment. The trochlear notch of the ulna reveals mild sclerosis caudal to the MCP. A moderate amount of osteophytes is seen at the pericarticular margins. The medial epicondylus of the humerus presents an ununited ossification center as well as moderate enthesiophytosis which is an incirect sign of flexor enthesiopathy. The subhcondral bone of the trochlea humeri is sclerotic but even and smooth with no obvious defects. Multifocal small well-delineated mineral opacities are seen within the soft tissue and likely foci of incidental dystrophic mineralization
RIGHT ELBOW: The right elbow presents very similar changes compared with the left one. However the radiogrpahic changes are slightly less pronounced
LEFT SHOULDER: A focal area of increased bone opacity is seen within the intertubercular groove.
CERVICAL SPINE: The cervical spine is within normal limits
The age of the patient is unusual for the first occurrence of clincial signs linked to medial coronoid pathology only. Late onset elbow dysplasia is typically associated with complex medial compartment syndrome with cartilage breakdown and activated synovialitis. In this case indirect signs of flexor origin enthesiopathy are seen as well which may also contribute to the lameness. Should the patient be refractory to medical treatment and physical therapy the further management should include pre- and post-contrast CT of both elbows as well as athroscopic revision of the affected joint.
R/O elbow dysplasia vs other