Presenting clinical signs: sudden onset of acute hind limb paralysis.
Presenting clinical signs: sudden onset of acute hind limb paralysis.
Presenting clinical signs: sudden onset of acute hind limb paralysis.
Presenting clinical signs: sudden onset of acute hind limb paralysis.
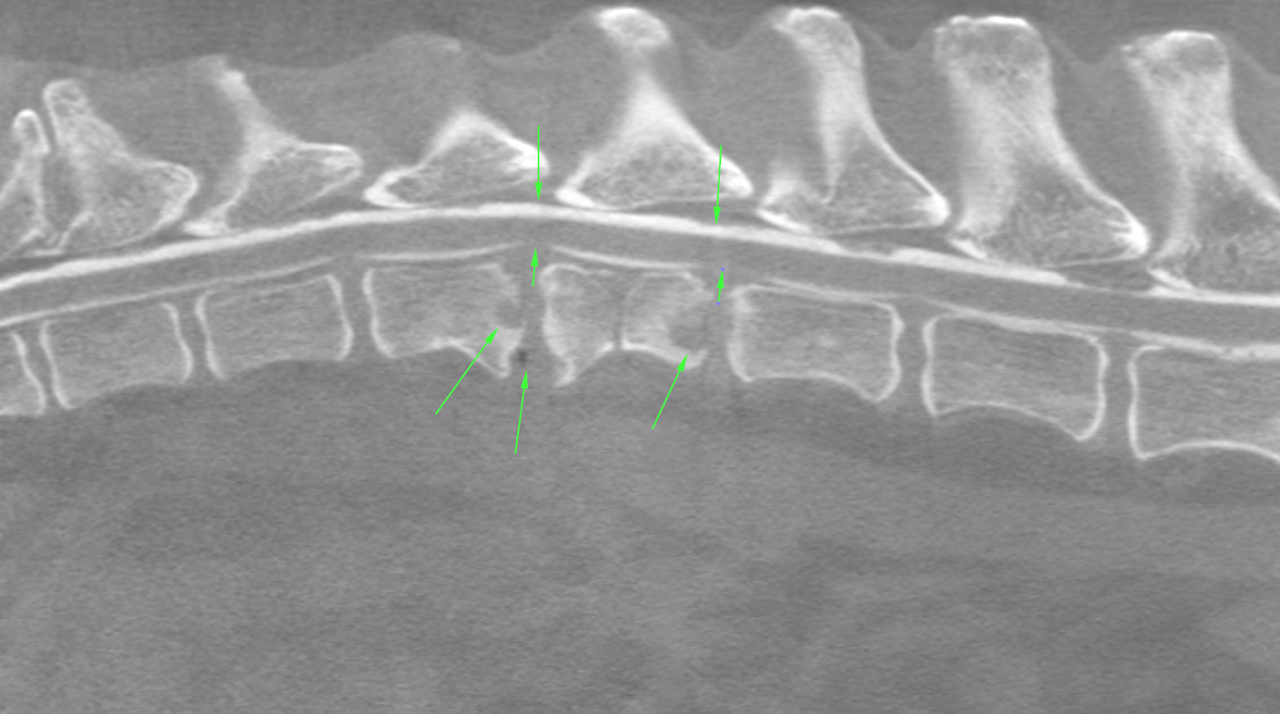
CT of the spine including T10 to sacrum: There were punched out osteolytic lesions within the neighboring vertebral endplates surrounded by a sclerotic margin level with T13/L1 and L1/L2. The respective discs presented moderate protrusion occupying the ventral epidural space. The dorsal subarachnoid contrast column was maintained throughout. Mild to moderate new bone formations were present emerging from the ventral aspect of the affected vertebral endplates. There was a small paravertebral vacuum phenomenon associated with the hypaxial muscles level with T13/L1.
A moderate disc protrusion was noted level with T12/T13.The ventral epidural space was occupied and the ventral contrast column was nearly lost. The dorsal contrast column was maintained.
A moderate disc protrusion was seen at the lumbosacral junction. There was moderate hypertrophy of the interarcuate ligament. The ventral epidural fat was lost. The dorsal epidural space was mildly reduced. The height of the left lumbosacral neuroforamen was mildly reduced at its exit zone by new bone formation emerging from the vertebral endplates.
Minor disc protrusions without signs of compressive myelopathy were present throughout the remainder of the imaged spine.
There were mild bilateral signs of coxofemoral joint osteoarthrosis as a function of mild hip dysplasia.
There was moderate generalized age related osteopenia.
|
Note that the presence of a maintained dorsal subarachnoid space indicates that the compressive effect on the spinal cord is only mild at present. Also the history of an acute onset does not parallel the imaging findings that clearly indicate chronicity.
|