History of respiratory difficulties. PE: increased respiratory rate (40); abominal breathing. CBC and Chem WNL.
History of respiratory difficulties. PE: increased respiratory rate (40); abominal breathing. CBC and Chem WNL.
History of respiratory difficulties. PE: increased respiratory rate (40); abominal breathing. CBC and Chem WNL.
History of respiratory difficulties. PE: increased respiratory rate (40); abominal breathing. CBC and Chem WNL.
right lateral, left lateral and VD thorax and abdomen: Osseous structures: There were moderate degenerative changes including
spondyloses level with the intervertebral disc spaces T11/12, L2/3.
Overall the degenerative changes associated with the axial sceleton were
mild to mdoerate.
Extrathoracic/-abdominal soft tissues: Within normal limits.
Abdominal Structures:
The serosal detail was normal.
The liver was within normal limits.
The stomach presented moderate aerophagia which likely was a function
of respiratory distress here.
Intrathoracic structures:
The esophagus was not seen.
The course of the trachea was normal.
There was no mediastinal widening and no evidence of mediastinal
lymph node enlargement. There was no mediastinal shift.
The cardiac silhouette was within normal limits. The major and
pulmonary vessels were within normal limits.
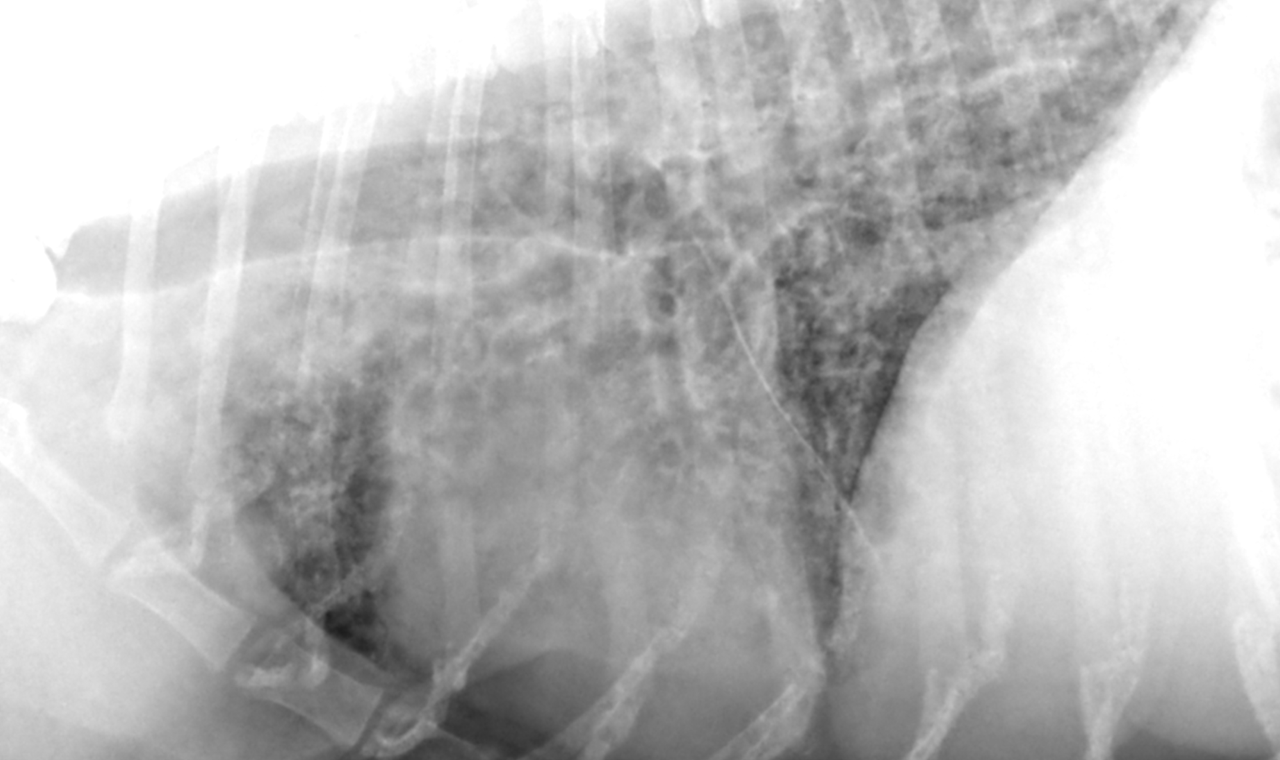
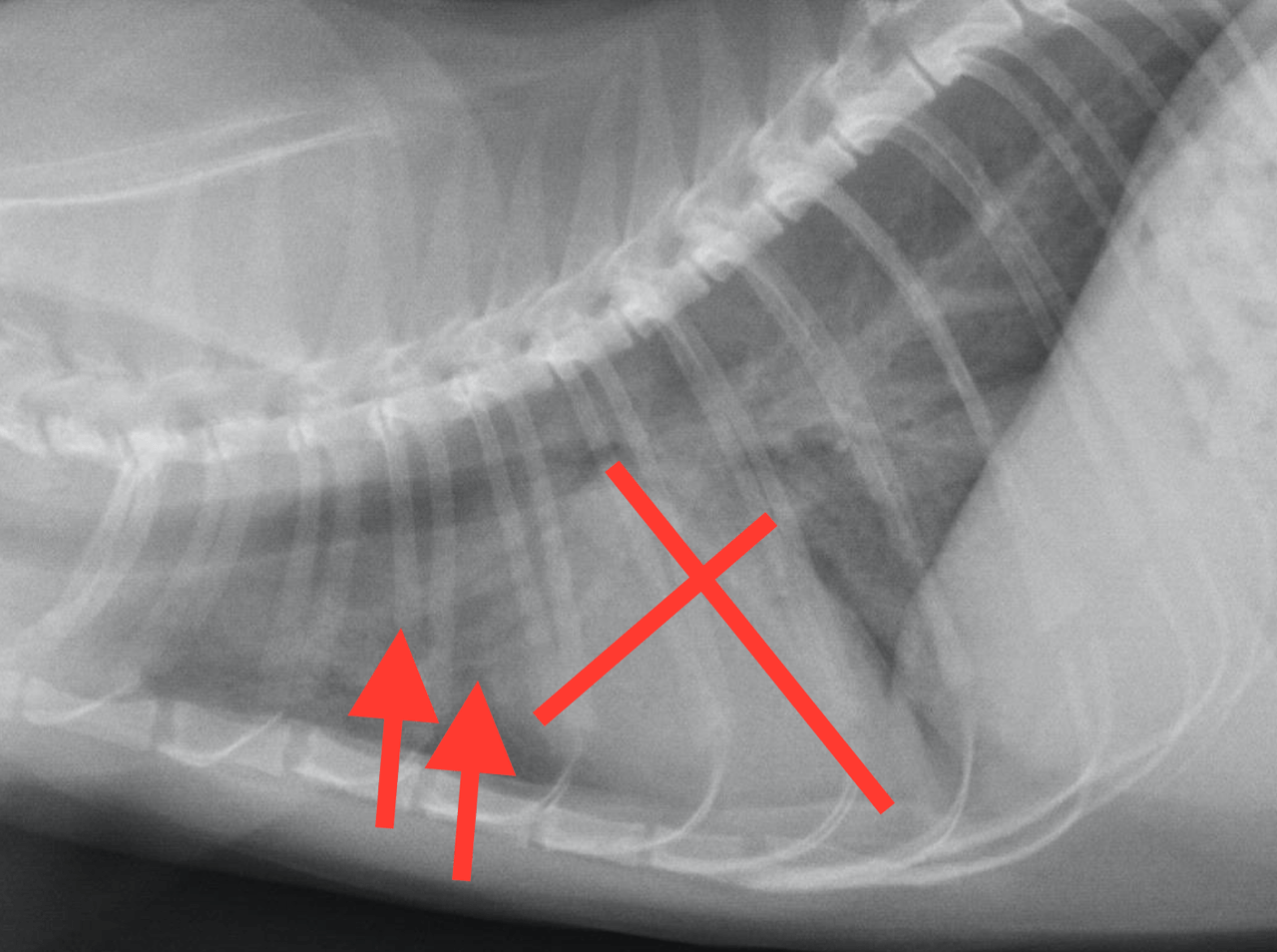
The lungs presented a severe generalized bronchoalveolar pattern with
peribronchial cuffing and confluent parenchyma consolidations. A
miliary pattern was noted in some areas. There was mild pleural
thickening and marked generalized bronchial wall mineralization.
Differentials include severe bronchitis – such as bacterial, funcgal or
mycobacterial as well as pulmonary infiltrates with eosinophils (usually
paralleled by marked peripheral eosinophilia). Typical cardiac changes in
heartworm infection are lacking here.
For further diagnostic workup abdominal ultrasound and echo of the heart
base level is recommended to rule out a possible primary neoplasia. If
this is negative bronchoscopy with bronchoalveolar lavage and
ultrasound guided fine needle aspiration of the lung parenchyma should
be enforced. Rule out lung worm infection by fecal exam.