History of GDV 2 days ago and post-op stomach tack. Physical exam found the patient with an increased respiratory rate
History of GDV 2 days ago and post-op stomach tack. Physical exam found the patient with an increased respiratory rate
History of GDV 2 days ago and post-op stomach tack. Physical exam found the patient with an increased respiratory rate
History of GDV 2 days ago and post-op stomach tack. Physical exam found the patient with an increased respiratory rate
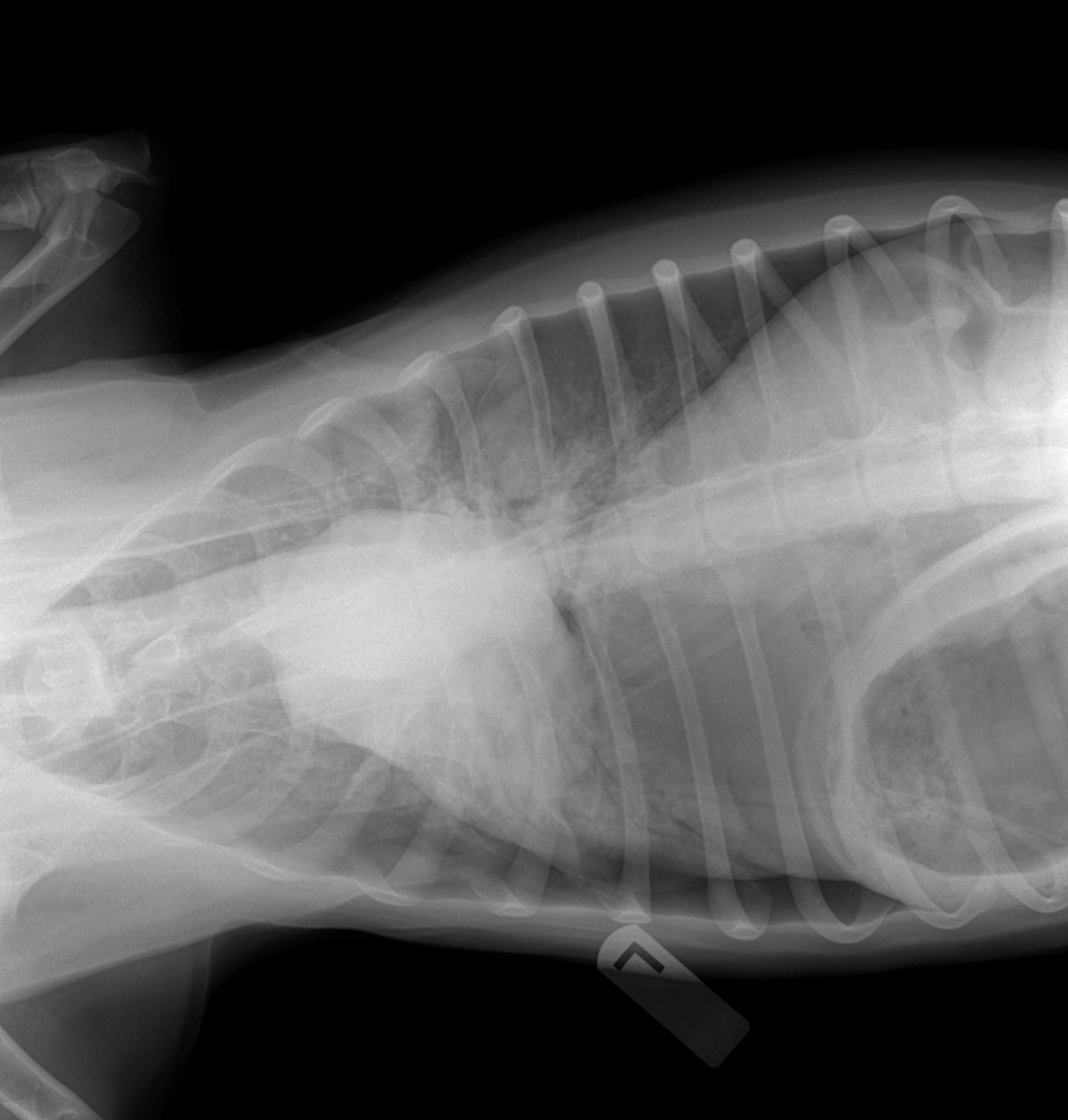
Pleural Space- There is retraction of the lung lobes seen especially in the left hemithorax. There is a mediastinal shift to the left and the heart apex is deviated to the left. This is somewhat exaggerated by obliquity of the dorsal ventral projection. Minimal to little air is noted on the right hemithorax. Lungs- There is increased lung opacity in the right middle, left middle and caudal lung fields. This is predominantly thought to be atelectasis; however, infiltrative disease cannot be exclusively ruled out.
Heart- The heart is thought to be small. This is consistent with hypovolemia or due to the previous surgery. Body Wall- No body wall defect was noted. Mediastinum- The esophagus, aorta and caudal vena cava are seen very well. This may be due to the pneumothroax or concurrent pneumomediastinum. However, no evidence of air surrounding the trachea is noted to indicate that the air that may be in the mediastinum is tracking up to or coming down from the neck region. Abdomen- A moderate amount of air was seen within the peritoneal space. This is consistent with a history of surgical repair of gastric dilation volvulus. There is concurrent loss of abdominal detail that is consistent with mild peritonitis or peritoneal free fluid, again associated with the previous surgery. Gastrointestinal Tract- There is heterogenous material within the stomach and fine bone opaque material thought to be in the pyloric canal. The remaining gastrointestinal tract is thought to be within normal limits. Urinary Tract- The urinary tract is thought to be within normal limits, although the single abdominal radiograph does not include the urinary bladder and additional structure more caudally.
Recommendations for the patient were as follows: Thoracocentesis to allow the lungs to re-expand and then repeat radiographs to evaluate the opacity and distribution of the lungs post removal of pleural free air. If the air continues to accumulate at a high rate and cause severe clinical signs, consider chest tubes. A chest tube in the left side would be the first indicated given the asymmetrical distribution. Since the cause of the pneumothroax is indeterminate based on these images, continue to evaluate the most opaque lungs, left, middle and caudal lungs for evidence of organic disease such as necrotizing tumor, pneumonia or other cavitated lesion not seen on these images. This will be better evaluated once the lungs re-expand post removal of pneumothroax.