A 10-year-old MN Elkhound dog with a history of chronically elevated liver values nd p[ast episodes of hepatitis. He presented for possible foreign body ingestion, protracted vomiting, anorexia, and decreased activity. Physical examination was non-remarkable. Urine specific gravity was within normal limits. Abnormalities on CBC and blood chemistry were leukocytosis, monocytosis, increased basophils, mild azotemia, hyperkalemia, elevated total protein, mild hyperalbuminemia, and elevated ALP activity.
A 10-year-old MN Elkhound dog with a history of chronically elevated liver values nd p[ast episodes of hepatitis. He presented for possible foreign body ingestion, protracted vomiting, anorexia, and decreased activity. Physical examination was non-remarkable. Urine specific gravity was within normal limits. Abnormalities on CBC and blood chemistry were leukocytosis, monocytosis, increased basophils, mild azotemia, hyperkalemia, elevated total protein, mild hyperalbuminemia, and elevated ALP activity. Radiographs showed urinary calculi, distended stomach, and a questionable pattern in the small intestines. The patient was treated with subcutaneous fluids, cerenia, and famotidine. exploratory surgery had been performed for GI foreign body and the sonogram was performed post-op.
Case Study
Gastritis, enteritis, post operative peritonitis with benign hepatic vacuolization in a 10 year old MN Elkhound dog
Sonographic Differential Diagnosis
Lobar liver swelling consistent with hepatoma or low grade neoplasia. Post operative peritonitis with potential perforation and adhesions.
Image Interpretation
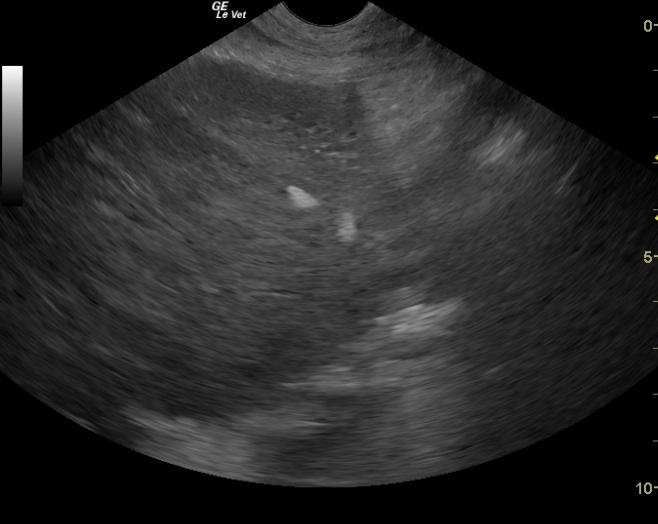
The liver presented swollen but regular contour and micronodular changes with reactive pericapsular omentum. Echogenic free fluid was present suggestive for hemorrhage or peritonitis. Adhesions along the small intestinal border are represented by hyperechoic fat attached to the intestinal serosa and move with the intestine.
DX
Outcome
Post surgery complications were ascites and a painful abdomen which improved within a few days with continuous supportive care and treatment with Buprenex, famotidine, Baytril, Cefazolin, I.V. fluids, and hetastarch. The patient was discharged a week later with Clavamox, metronidazole, famotidine, Carafate, and a bland diet. Recheck ultrasound five days later showed a small amount of ascites. As there was a concern of possible perforation, an exploratory surgery was recommended with abdominal lavage. The owner elected to continue medical treatment at home and a follow-up ultrasound a few days later showed no free fluid in the abdomen.
Comments
This is one of those “give the patient the benefit of the doubt” cases. The peritonitis itself resolved with outpatient therapy. Obviously repeat exploratory was the treatment of choice.
Clinical Differential Diagnosis
GI pathology- foreign body, neoplasia, intussusception, torsion, IBD, peritonitis. Early renal disease
Sampling
Gastrointestinal biopsies had been performed at the time of the original exploratory. A fabric gastric foreign body had been removed from the stomach. Surgical biopsies of the liver revealed hepatopathy, characterized by hepatocellular swelling, hepatocellular vacuolation, and mild portal inflammation. Sections of the stomach revealed moderate chronic gastritis. Sections of the small intestine revealed moderate sub-acute to chronic enteritis.
Video
Patient Information
Clinical Signs
- Anorexia
- Concern for FB Ingestion
- Lethargy
- Vomiting
Images
Blood Chemistry
- Albumin, High
- Alkaline Phosphatase (SAP), High
- Azotemia
- Potassium, High
- Total Protein, High
CBC
- Basophils, High
- Monocytes, High
- WBC, High
Clinical Signs
- Anorexia
- Concern for FB Ingestion
- Lethargy
- Vomiting