This 15 year old FS French Bulldog has a 3 week history of coughing. CBC/Chem: CK 275, Amyl 1499, BUN 42, Crea 1.5. UA: USPG 1.018, WBCs and RBCs present; marked bacteria
Case Study
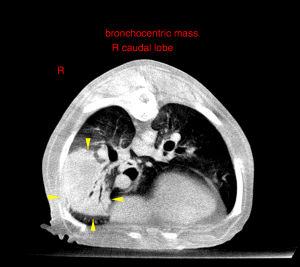
CT – Caudal lung lobe mass, splenic mass and renal cysts in a 15 year old FS French Bulldog
Image Interpretation
CT of the thorax and abdomen-
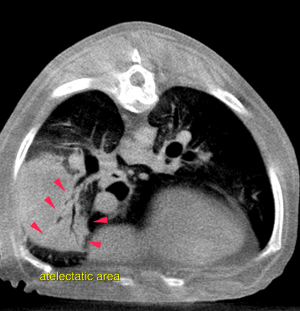
The ventral aspect of the right caudal lung lobe presents a well-delineated bronchocentric, moderately contrast enhancing soft tissue attenuating mass lesion, measuring 56 x 46 x 46 mm in size. Partial collapse of the encompassed bronchi is noted. The ventral margin of the right caudal lung lobe is rounded. A small mineralized area is noted within the mass lesion. The lung parenchyma situated cranioventral to the mass lesion presents homogeneous soft tissue attenuation and a marked reduced volume with air-bronchograms. The bronchial walls of the right cranial, middle, caudal and accessory lung lobe present moderate broncho-centric thickening. One second degree bronchus of the right middle lung lobe presents complete collapse with secondary soft tissue attenuation and reduced volume of the associated lung parenchyma.
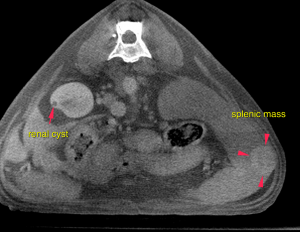
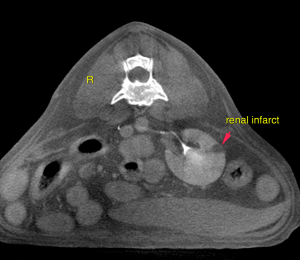
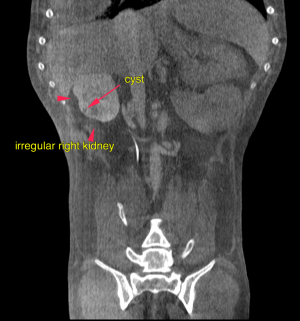
The right kidney was small with an irregular shape. After contrast administration both kidneys present multiple triangular shaped contrast sparing defects and multiple small cystic lesions. The spleen presents prominent with rounded margins. A moderately irregular contrast enhancing mass lesion of 1.6 cm diameter is seen with bulging of the splenic capsule within the splenic tail.
DX
Soft tissue neoplasia right caudal lung lobe, compatible with primary or secondary neoplastic disease
Outcome
Possible differential diagnoses include broncho-alveolar carcinoma, squamous cell carcinoma, round-cell neoplasia (lymphoma, histolytic sarcoma) or metastatic disease in the context of the splenic mass lesion. The thickened bronchial walls are likely to be an expression of secondary lower airway obstruction rather than a diffuse neoplastic infiltration. The larger splenic lesion is suggestive for a neoplasia, which can either be malignant (hemangiosarcoma, fibrosarcoma, metastasis) or benign (hemangioma, benign nodular hyperplasia). The odds of the multiple smaller nodules being non-neoplastic lesions (nodular hyperplasia, extramedullary hematopoiesis) are considered high.
Patient Information
Gender :
Female, Spayed
Species :
Canine
Type of Imaging : CT
Exam Finding
- Amylase
- Bacteria Present
- BUN high
- Coughing
- High
- Specific Gravity Low
- WBCs Present Amylase
Images