A 12-year-old SF DSH was presented for evaluation of elevated liver enzyme activity and cranial organomegaly.
A 12-year-old SF DSH was presented for evaluation of elevated liver enzyme activity and cranial organomegaly.
A 12-year-old SF DSH was presented for evaluation of elevated liver enzyme activity and cranial organomegaly.
A 12-year-old SF DSH was presented for evaluation of elevated liver enzyme activity and cranial organomegaly.
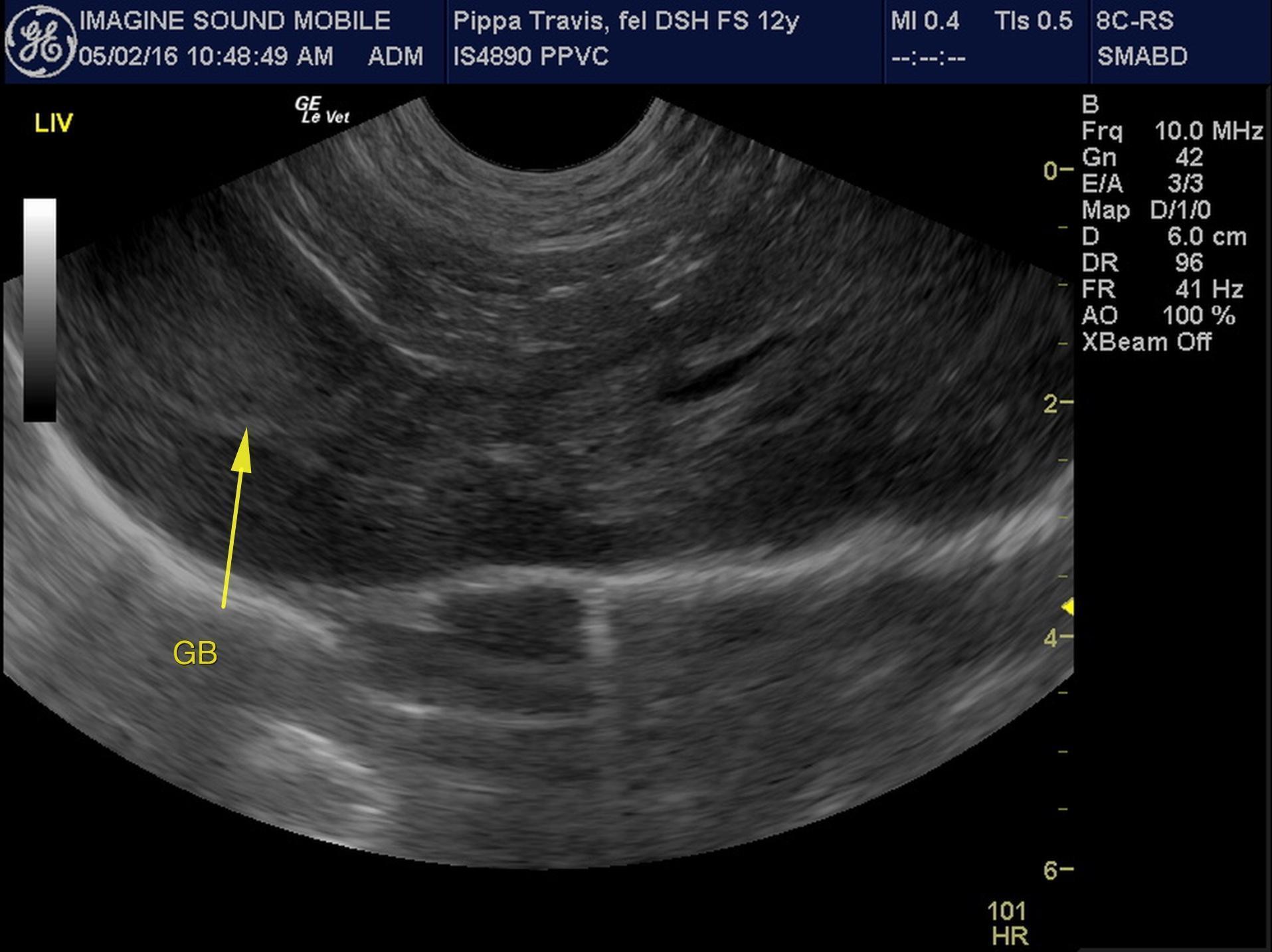
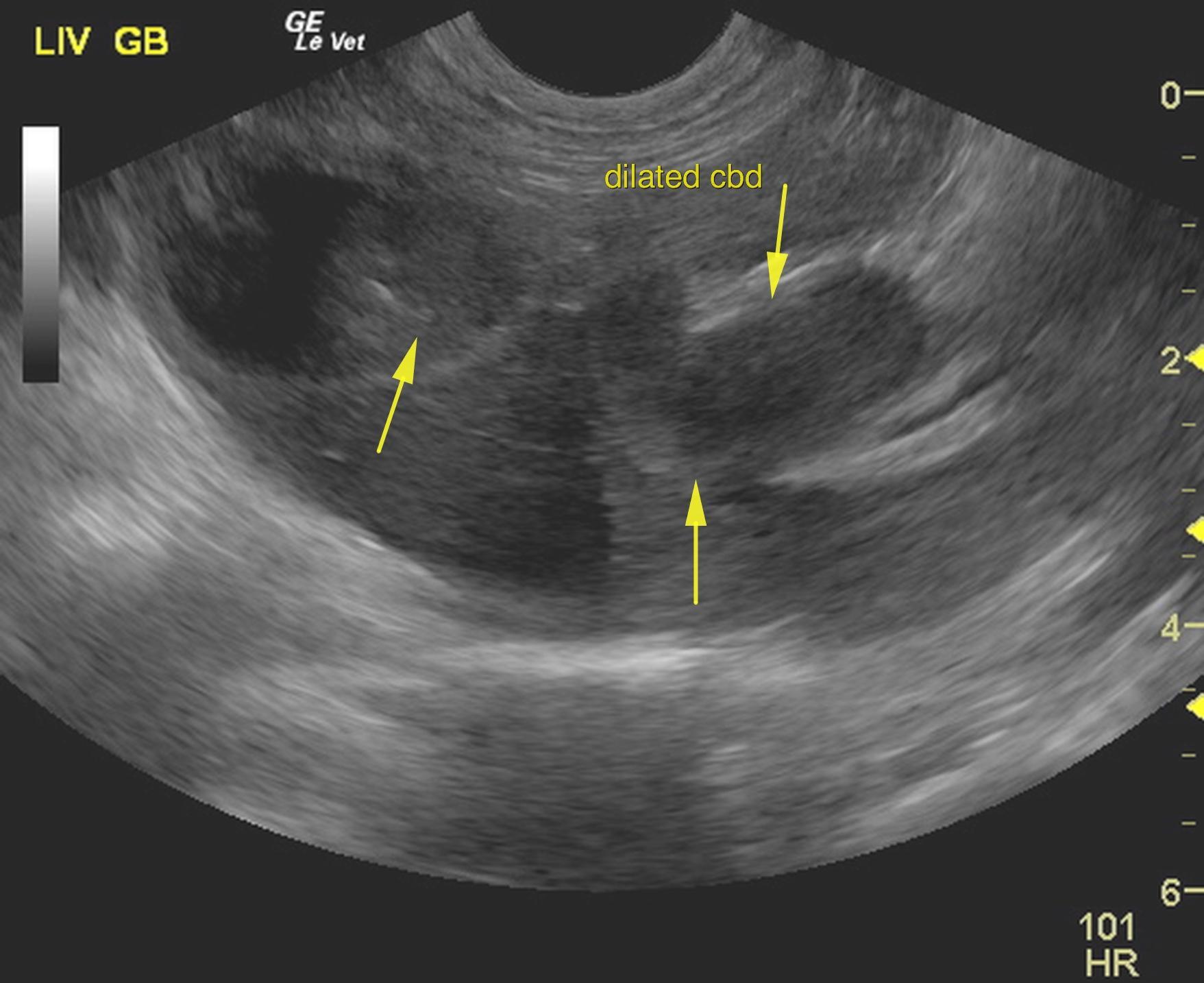
Mild hepatomegaly was noted. The hepatic parenchyma was course with increased portal markings. The gallbladder presented excessive debris and minor, over distension along with a thickened wall. The common bile duct was severely dilated and thickened in this patient. The common bile duct measured 1.0 cm in width with echogenic debris and over distension. This continued into the union of the pancreatic duct, which was also distended. Lobar biliary duct dilation was noted.
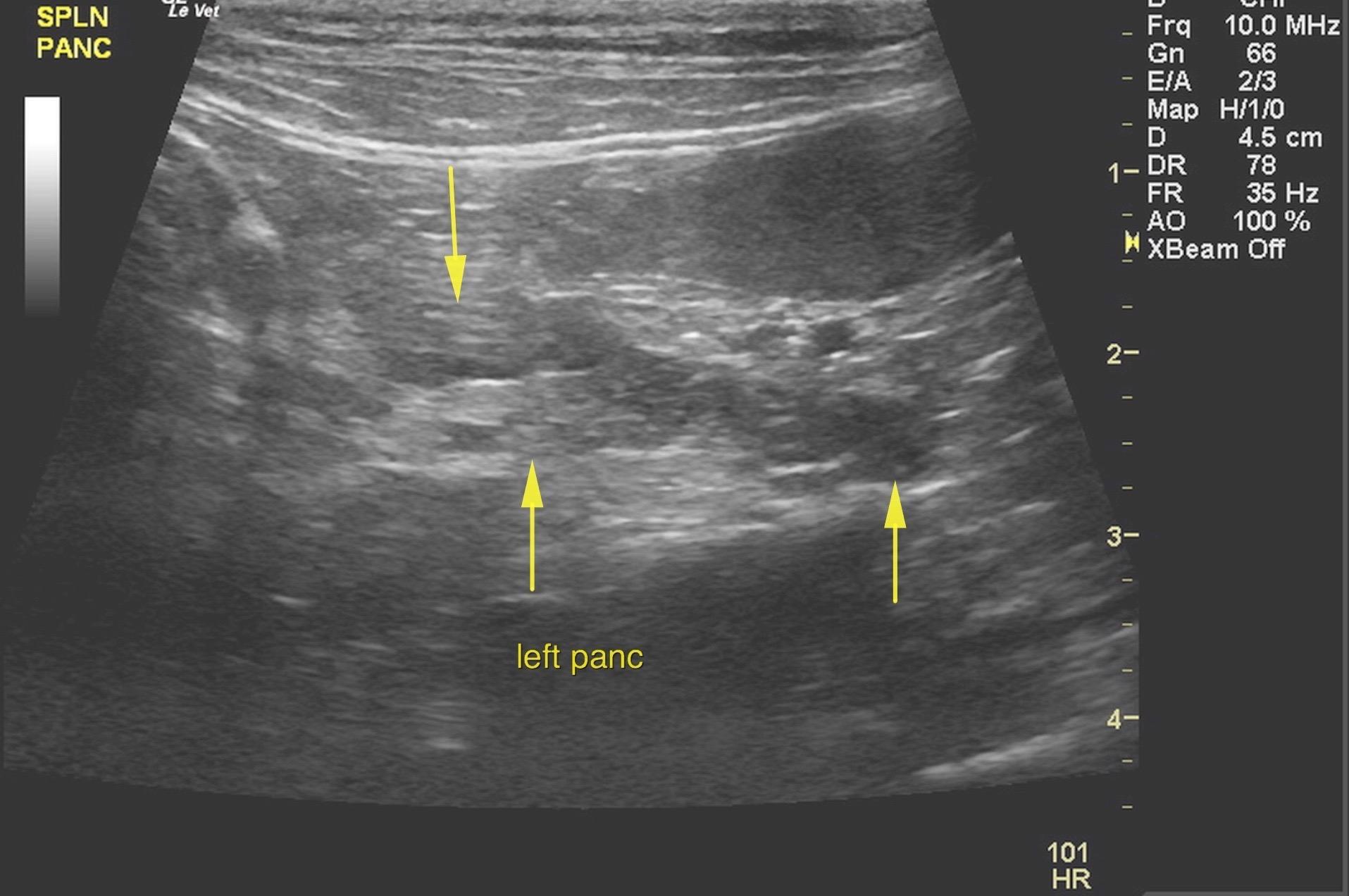
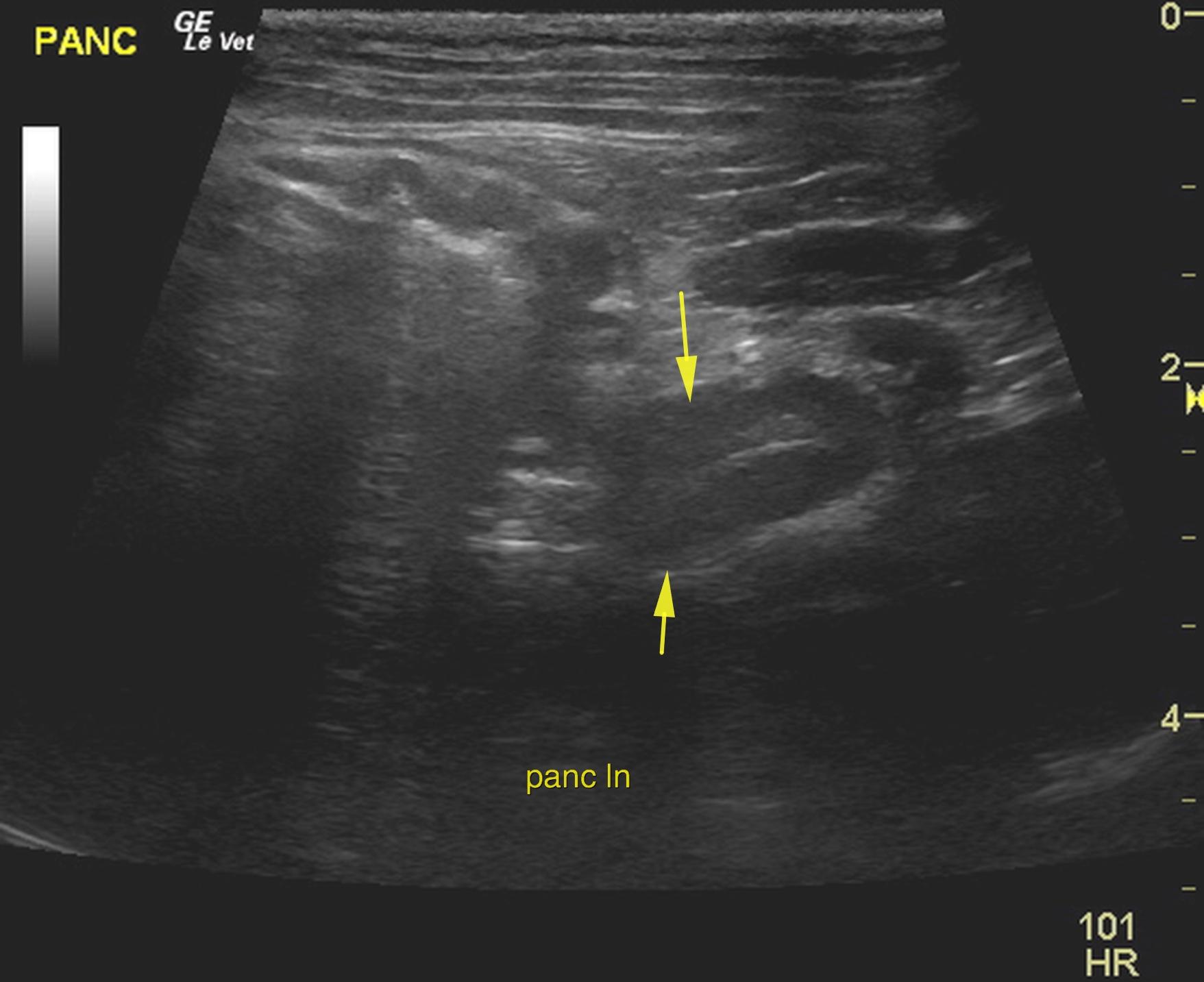
The pancreas was enlarged, hypoechoic and irregular with undulating contour. Irregular, hypoechoic parenchyma was noted throughout the right limb of the pancreas as well with ill defined surrounding fat. This is strongly suggestive for pancreatitis with a potential for underlying pancreatic carcinoma. Pancreatic lymph node was enlarged and measured 1.0 x 1.5 cm.
Lobar biliary duct dilation was also noted.
Post hepatic obstruction owing to pancreatitis, potential underlying pancreatic carcinoma. Surgical intervention is strongly recommended in this patient with expectations towards cholecystoduodenostomy. Appropriate biopsies are also warranted. There was no obvious evidence of neoplasia. However, carcinoma can present in this manner. This is likely chronic pancreatitis, cholangitis with dysfunctional common bile duct and gallbladder with inspissated debris. Guarded prognosis depending on response to surgical intervention.
Liver – cholangio-hepatitis complex, lipidosis, neoplasia
Pancreas – neoplasia, cyst
Cyst/neoplasia/abscess – mesentery, lymph node