A 15-year-old MN Malti-poo was presented for progressive lethargy, anorexia, and weight loss. Physical exam found patient icteric, with a painful cranial abdomen. Blood chemistry revealed mild hyperglycemia, hyperbilirubinemia, hypercholesterolemia, elevated Alkaline Phosphatase, high ALT, high AST, and high GGTP. CBC found leukocytosis, neutrophilia, high bands, monocytosis and high platelet count.
A 15-year-old MN Malti-poo was presented for progressive lethargy, anorexia, and weight loss. Physical exam found patient icteric, with a painful cranial abdomen. Blood chemistry revealed mild hyperglycemia, hyperbilirubinemia, hypercholesterolemia, elevated Alkaline Phosphatase, high ALT, high AST, and high GGTP. CBC found leukocytosis, neutrophilia, high bands, monocytosis and high platelet count.
Case Study
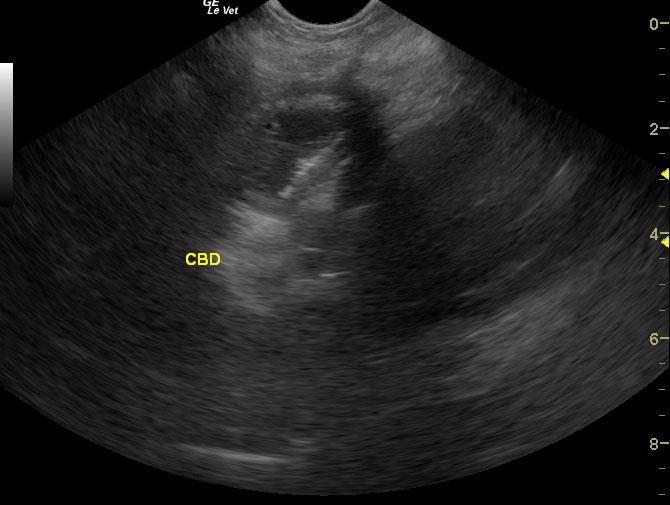
Perforating GB mucocele with thickened common bile duct (CBD) and pancreatitis in a 15 year old MN Maltese-Poodle mix dog
Sonographic Differential Diagnosis
Perforating gallbladder mucocele. Thickened common bile duct. Guarded prognosis.
Image Interpretation
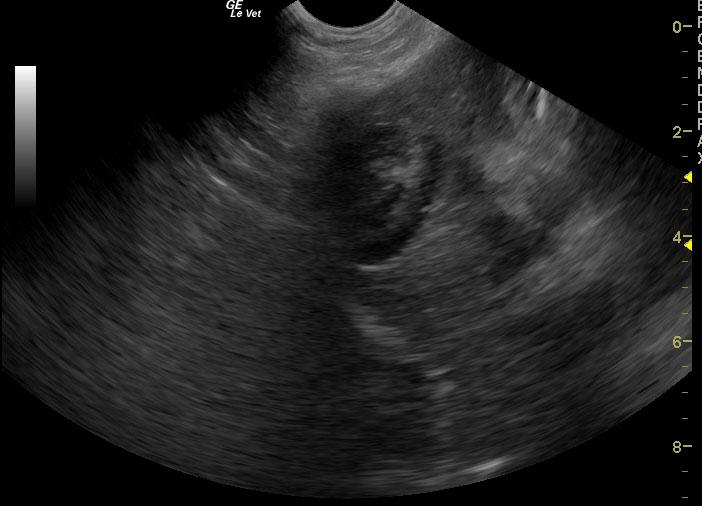
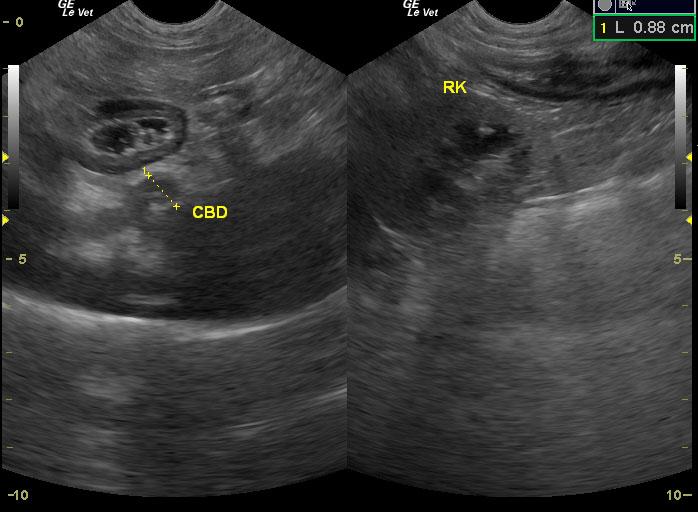
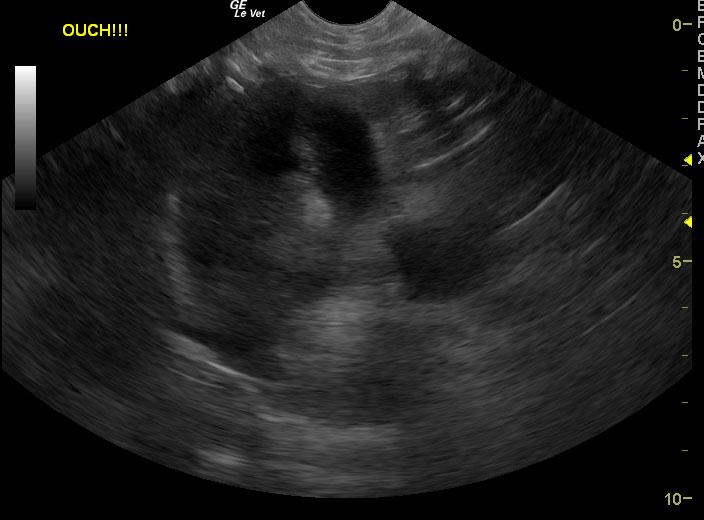
The liver presented swollen contour with heterogenic changes and increased portal markings. The gallbladder was dilated at 5cm with suspended debris and echogenic fat with a positive Murphy sign and minor free fluid associated with a double wall gallbladder and likely perforated cystic duct consistent with localized bile peritonitis. Often the right intercostal approach evidences the GB dilation and mucocele aspects more so than the subxyphoid approach. Dilated common bile duct with sludge material was also noted consistent with chronic biliary congestion.
DX
Outcome
Cholecystectomy, liver biopsy, common bile duct (CBD) lavage, with possible urine culture and sensitivity if warranted was recommended. Patient was euthanized.
Comments
This GB mucocele is not particularly large but all aspects of an inflamed mucocele formation were present: Immobile suspended debris, dilation of the neck, + Murphy sign, and echogenic surrounding reactive fat. For more information on mucocele formation and clinical approach see our survey of clinical sonographers on the home page of sonopath.com or in resources. http://www.sonopath.com/resources_instructional.asp
Clinical Differential Diagnosis
Liver pathology: hepatitis- infectious, inflammatory, hepatopathy- toxic, metabolic, biliary mucocele, extrahepatic bile duct obstruction, cholecystitis; Pancreatic pathology: pancreatitis, infection, neoplasia.
Sampling
None taken.
Video
Media error: Format(s) not supported or source(s) not found
Download File: http://sonopath-videos.s3.amazonaws.com/sites/default/files/case_studies/videos/converted/03_00106_video_01_09082011030205.mp4?_=1Media error: Format(s) not supported or source(s) not found
Download File: http://sonopath-videos.s3.amazonaws.com/sites/default/files/case_studies/videos/converted/03_00106_video_02_09082011030322.mp4?_=2Media error: Format(s) not supported or source(s) not found
Download File: http://sonopath-videos.s3.amazonaws.com/sites/default/files/case_studies/videos/converted/03_00106_video_03_09082011030354.mp4?_=3Patient Information
Clinical Signs
- Anorexia
- Lethargy
- Weight loss
Exam Finding
- Abdominal Pain
- Icterus
Images
Blood Chemistry
- Alkaline Phosphatase (SAP), High
- ALT (SGPT), High
- AST (SGOT), High
- Cholesterol, High
- GGT High
- Glucose, High
- Total Bilirubin, High
CBC
- Monocytes, High
- Neutrophils, High
- Platelet Count, High
- WBC, High
Clinical Signs
- Anorexia
- Lethargy
- Weight loss