This 10-year-old FS Boxer had originally been presented for a routine screening for a dental prophylaxis procedure. The physical exam had been normal at that time. However, due to mildly elevated amylase and lipase on the preanesthetic screening, a sonogram. A left limb pancreatic mass (6 cm diameter) had been reported, but initially sampling had been declined by the owner. The images presented here were taken 4 months later, after abdominal palpation now revealed a thickening in the mid-abdomen.
This 10-year-old FS Boxer had originally been presented for a routine screening for a dental prophylaxis procedure. The physical exam had been normal at that time. However, due to mildly elevated amylase and lipase on the preanesthetic screening, a sonogram. A left limb pancreatic mass (6 cm diameter) had been reported, but initially sampling had been declined by the owner. The images presented here were taken 4 months later, after abdominal palpation now revealed a thickening in the mid-abdomen. Repeat blood analysis revealed moderately elevated amylase and lipase without other significant findings. The CBC was normal. Weight loss was not reported.
Case Study
Pancreatic cyst and neuroendocrine neoplasia diagnosed on ultrasound-guided FNA in a 10 year old FS Boxer
DX
Sonographic Differential Diagnosis
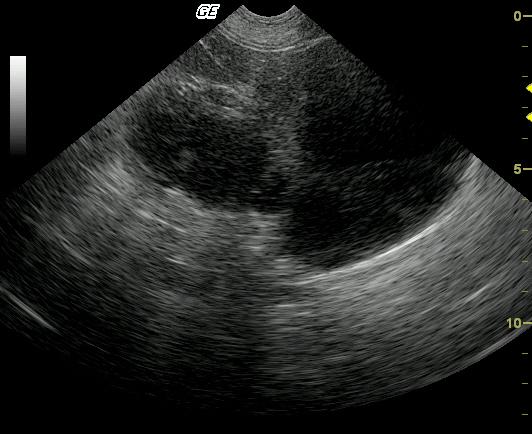
Cystic pancreatic mass, suspected areas of necrosis and cystic degeneration. Carcinoma is also possible.
Image Interpretation
The mid abdomen demonstrated large cystic structures deriving from the left pancreas with focal areas of hyperechoic mineralizing tissue. This is consistent with chronic pancreatic sequestrum with the possibility of emerging carcinoma. Video clip through the left sided pancreatic mass demonstrates echogenic parenchymal proliferation with focal dystrophic mineralization and large cystic changes that were subsequently drained (video 1). The mass appears largely resectable and did not extend into the gastrointestinal outflow. However, the mass did occupy the majority of the pancreatic base and left pancreatic limb.
Outcome
The bulk of the pathology was localized to the left pancreatic limb and base. The right pancreatic limb and area of the upper gastrointestinal outflow, pancreatic and common bile ducts were not affected. This, along with the slow insidious progression of this tumor would explain why the patient had been asymptomatic for so long given that no significant organ system was directly affected and enough residual pancreatic tissue was available to maintain homeostasis in this patient. The patient was imaged again at 2 months post sampling and the cysts had returned with mild increase in pancreatic size. The patient was still asymptomatic. Four months after the original presentation, the patient presented with dramatic weight loss and inappetance. Exploratory surgery was performed revealing diffuse abscessation of the cystic pancreatic mass. The owner selected humane euthanasia at surgery.
Clinical Differential Diagnosis
Chronic pancreatitis, active pancreatitis, pancreatic neoplasia, extra pancreatic neoplasia.
Sampling
A 22-gauge US-guided FNA of the abnormal parenchymal portion (obtained adjacent to the area of mineralization) revealed neuroendocrine neoplasia with chronic inflammation, necrosis, and hemorrhage. Concurrent 18-gauge catheter drainage of the cystic portion of the pancreas revealed a modified transudate with low grade degenerate neutrophils consistent with a pancreatic cyst.
Video
Patient Information
Clinical Signs
- Palpable Mass
History
- Abdominal mass
Images

Blood Chemistry
- Amylase, High
- Lipase, High
Clinical Signs
- Palpable Mass