History of collapse, cyanosis, left-sided cardiomegaly (on radiographs) and tracheal collapse. BP 111/80.
History of collapse, cyanosis, left-sided cardiomegaly (on radiographs) and tracheal collapse. BP 111/80.
History of collapse, cyanosis, left-sided cardiomegaly (on radiographs) and tracheal collapse. BP 111/80.
History of collapse, cyanosis, left-sided cardiomegaly (on radiographs) and tracheal collapse. BP 111/80.
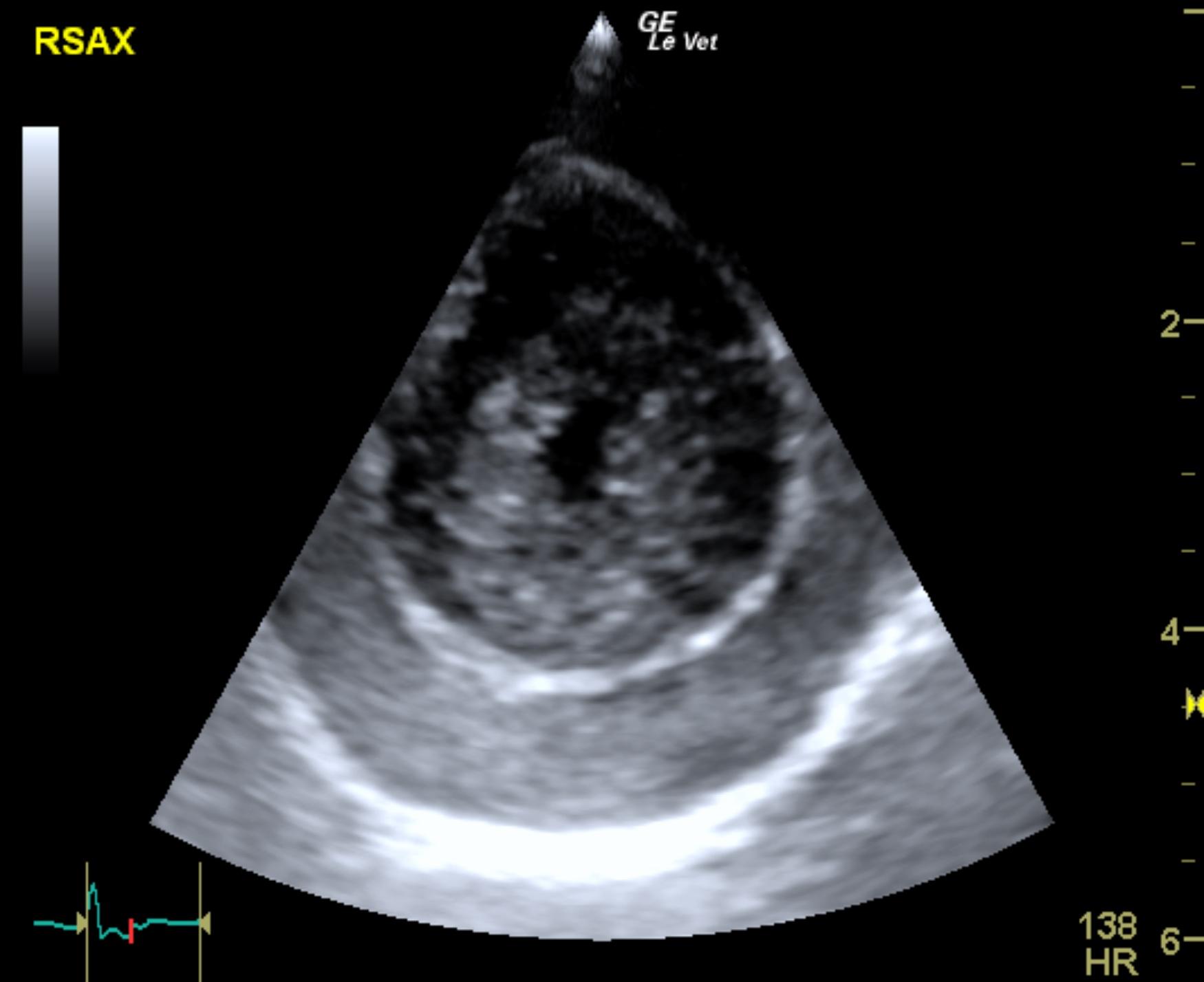
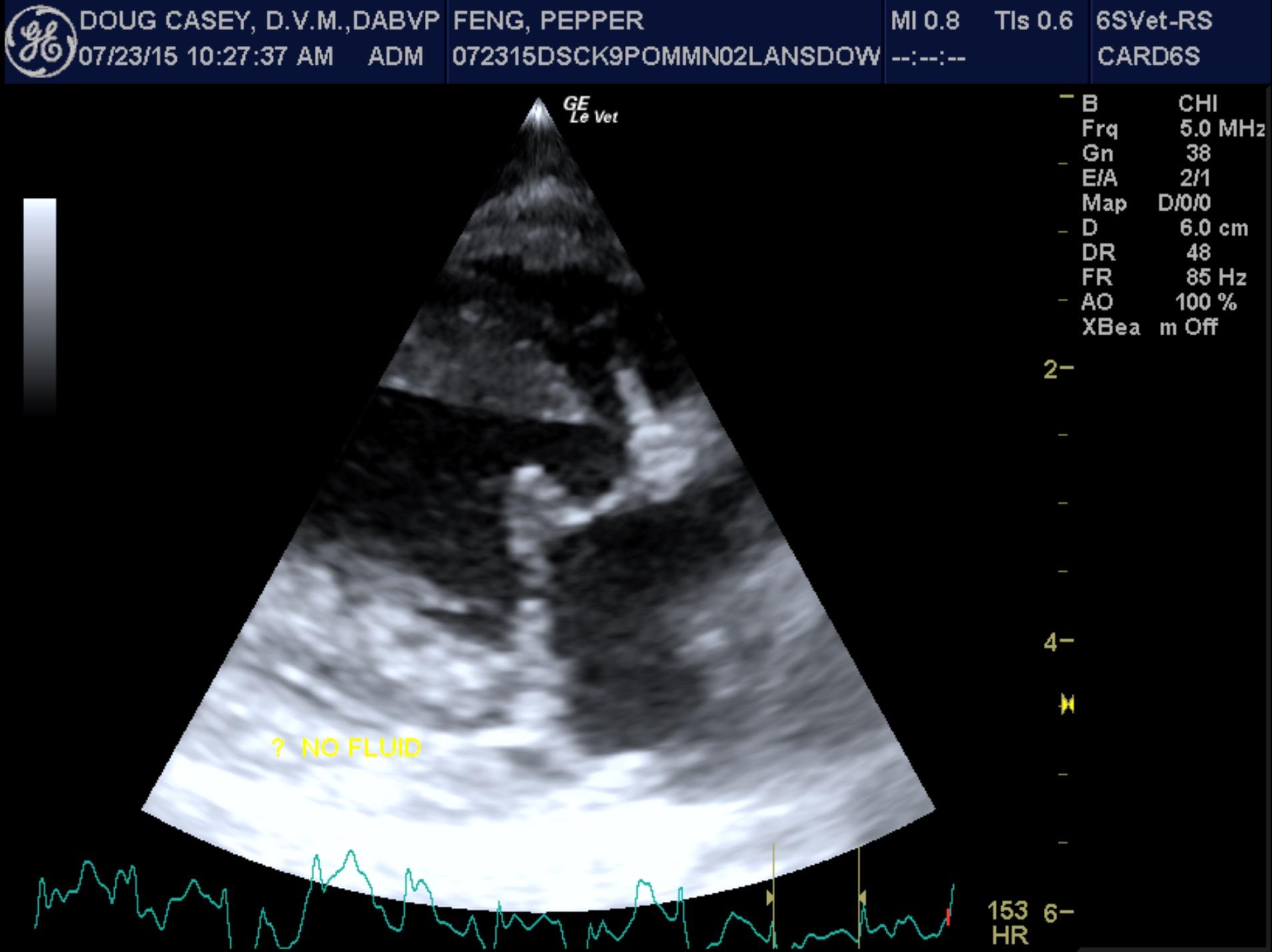
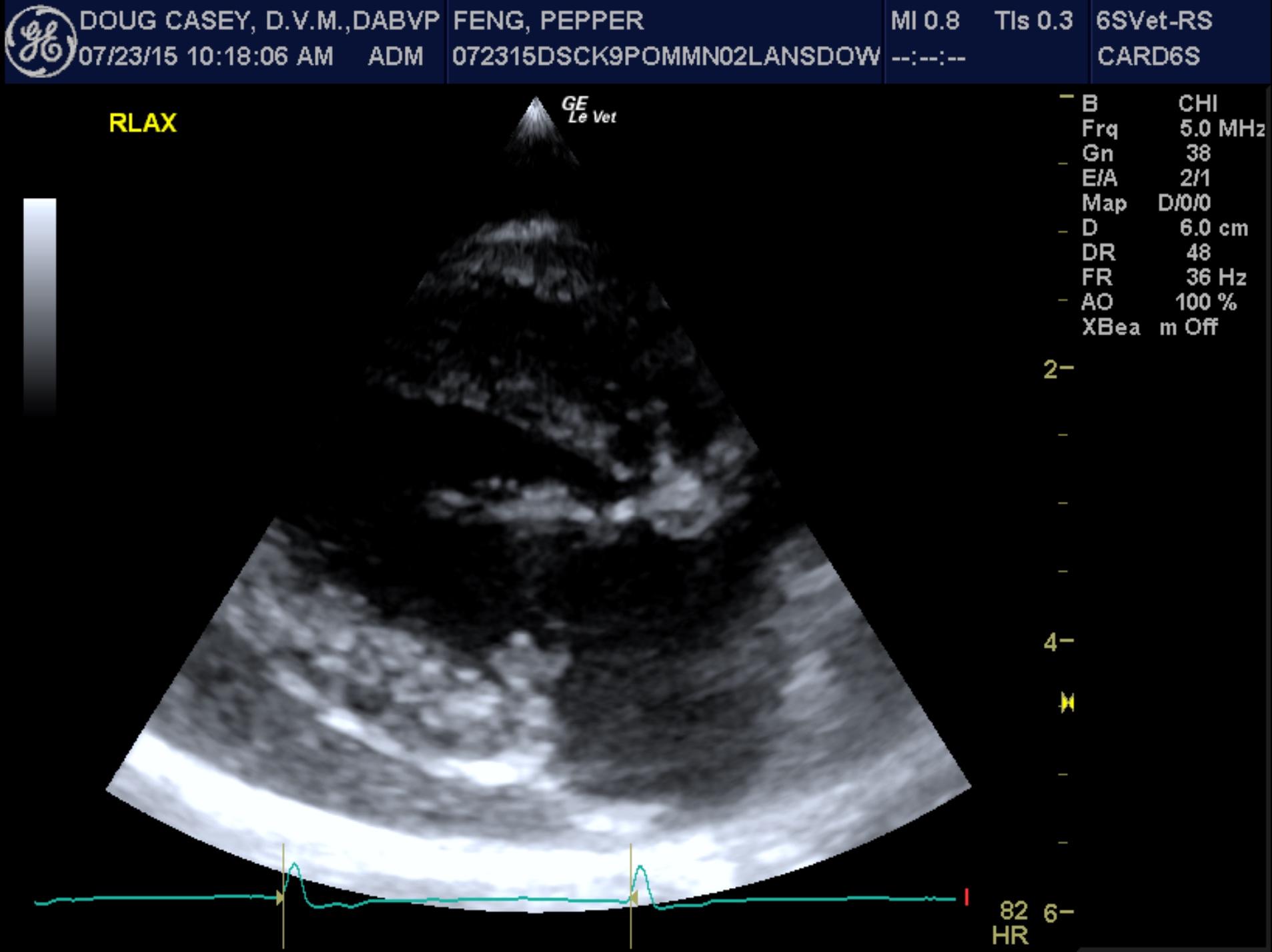
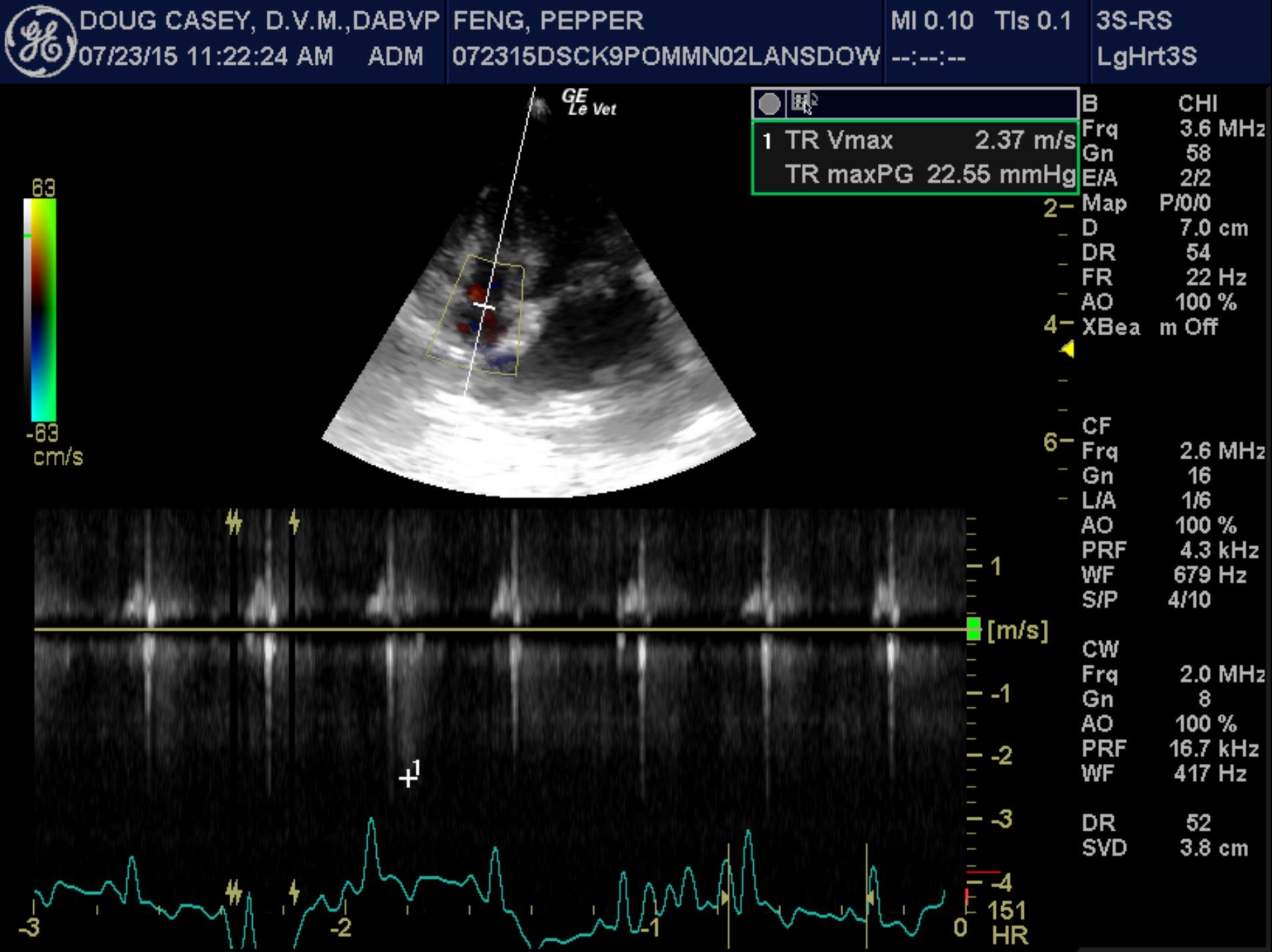
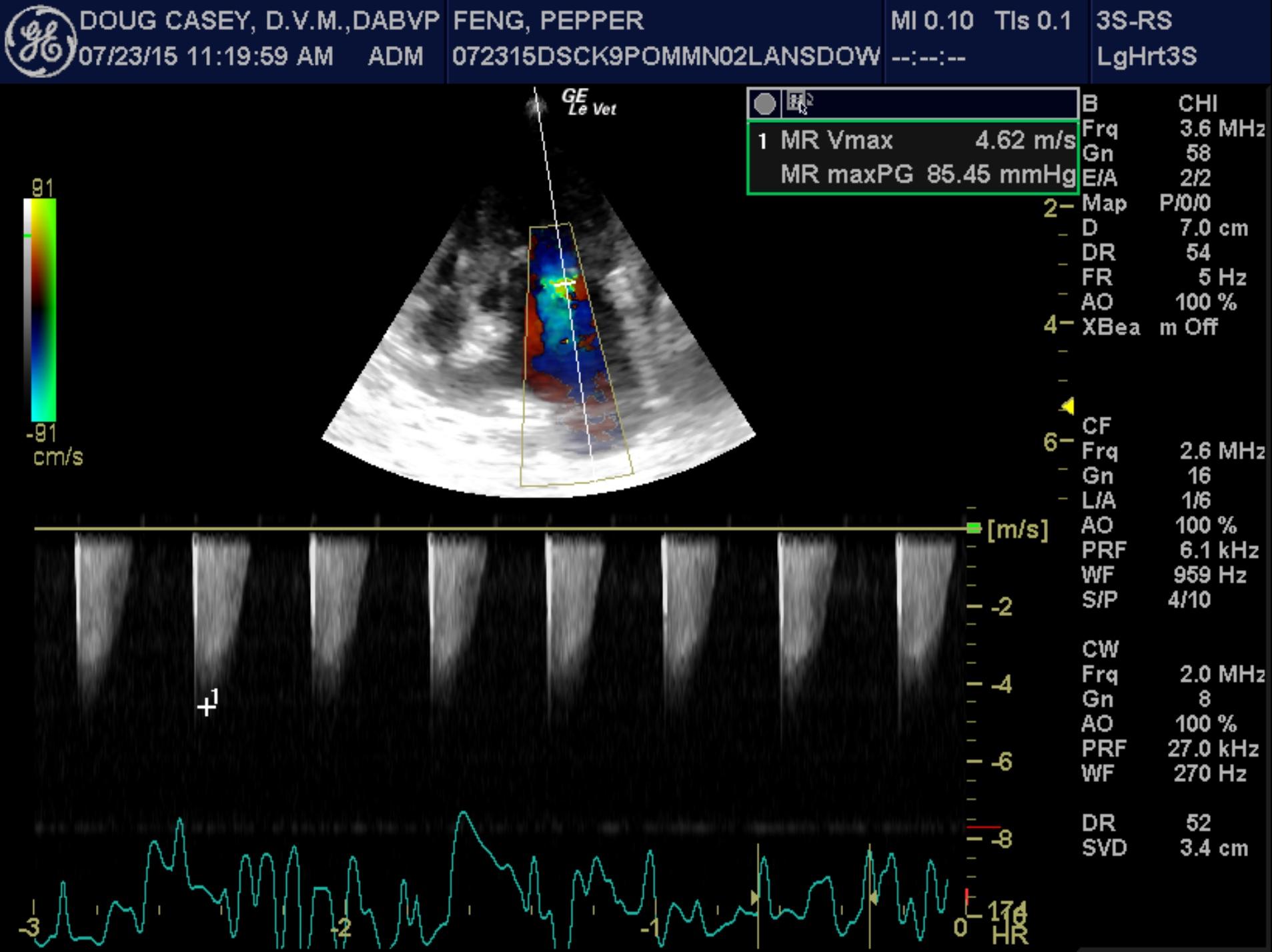
There is moderate left atrial enlargement. The mitral valve leaflets are thickened and exhibit systolic prolapse. A moderate jet of eccentric mitral regurgitation directed toward the left atrial free wall is present. Left ventricular dimensions are normal. Left ventricular systolic function is hyperdynamic. The left ventricular posterior wall and papillary muscles appear hyperechoic in relation to the interventricular septum. There is a mild to moderate pericardial effusion present, whose appearance is of mixed echogenicity, suggesting a high protein or cellular content. Right atrial and right ventricular dimensions are normal, though there is diastolic collapse of the right atrial wall secondary to the pericardial effusion. The tricuspid valve appears normal, though very mild tricuspid regurgitation is present. The pulmonary artery and pulmonic valve are normal, though trace physiologic pulmonic insufficiency is present. No distinct cardiac masses are seen.
LA – 25.7 mm
LVIDd – 19.5 mm
LVIDs – 7.9 mm
FS – 59%
LVOT Vmax – 0.80 m/s
RVOT Vmax – 0.50 m/s
TR – 2.39 m/s
This examination demonstrates multiple abnormalities. First, there is moderate mitral regurgitation and left atrial enlargement secondary to degenerative mitral valve disease. Secondly, there is mild to moderate pleural effusion present, an uncommon finding in small breed dogs. Given the presence of a jet of mitral regurgitation directed toward the left atrial free wall, it’s possible that the patient could have experienced a left atrial tear that has resulted in his pericardial effusion. Alternatively, his left ventricular posterior wall and papillary muscles are hyperechoic, which could potentially indicate infiltrative disease such as lymphoma as a cause of the pericardial effusion. Finally, it’s possible that the effusion could be idiopathic, though this is rare in small breed dogs.
While the absence of cardiac chamber underfilling and normal blood pressure suggest that cardiac tamponade is not present, the presence of right atrial diastolic wall collapse and clinical signs compatible with tamponade suggest that the pericardial effusion needs to be removed. There is a risk with pericardiocentesis, however, if a left atrial tear is present, as the relief of pressure on the left atrial wall that is achieved via removal of the pericardial effusion could allow for further bleeding through the tear, which could potentially be fatal. Having said that, obtaining even a small sample of the effusion for fluid analysis and cytology could potentially be very beneficial, as it may provide a more definitive cause of the effusion. Additionally, removal of the effusion may be required to relieve the clinical signs of cyanosis and collapse.
RECOMMENDATIONS:
Remove a small amount of effusion at first, just enough for fluid analysis and cytology, as long as the patient’s clinical status remains stable, so that we can potentially discover a cause of the effusion. Should the effusion not be caused by a left atrial tear, further pericardiocentesis to remove as much fluid as possible is recommended. If the fluid analysis is inconclusive, it is believed that repeat pericardiocentesis is warranted given the clinical signs, though extra caution must be used, as a severe acute increase in the amount of effusion can develop in the case of a left atrial tear.