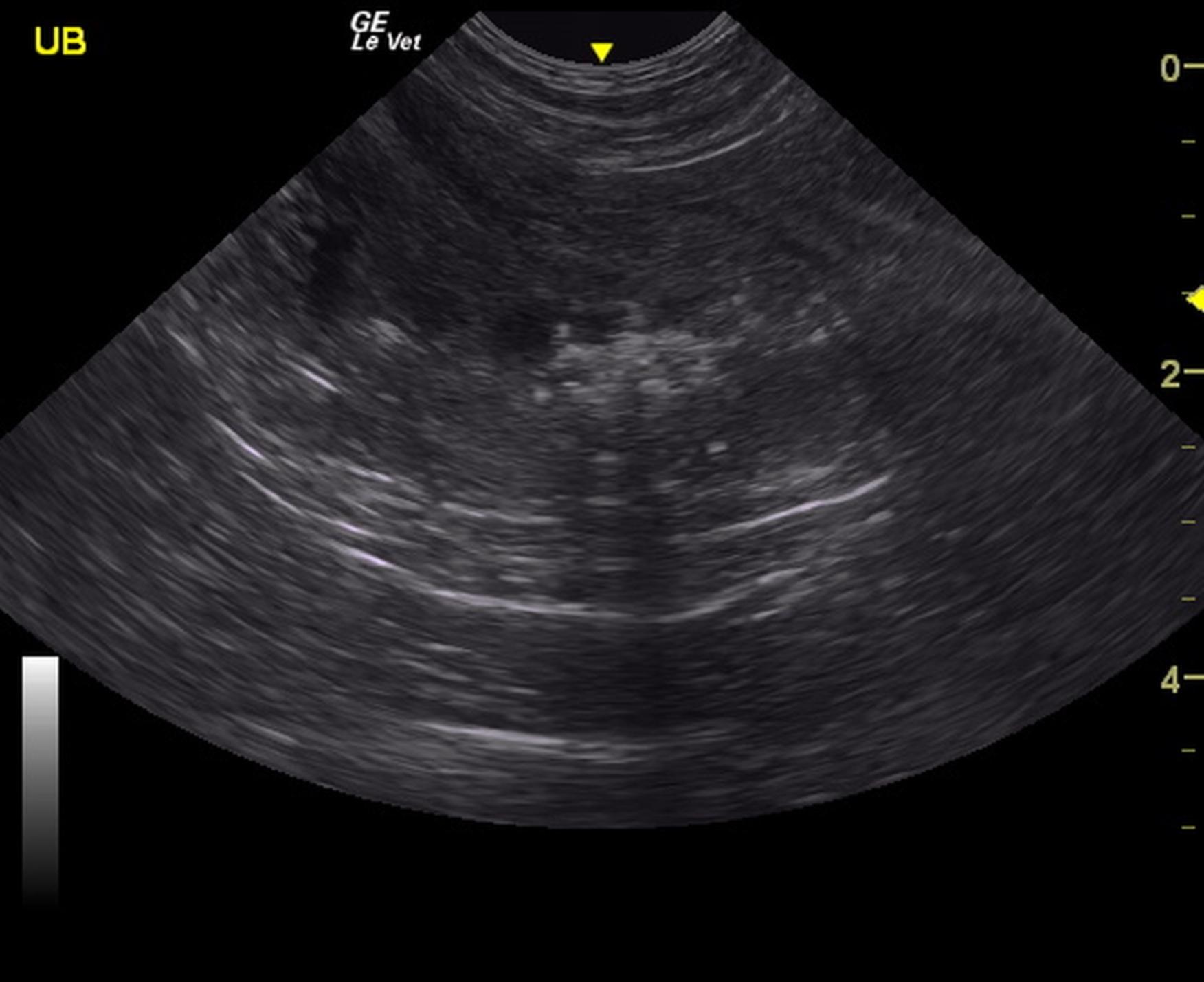
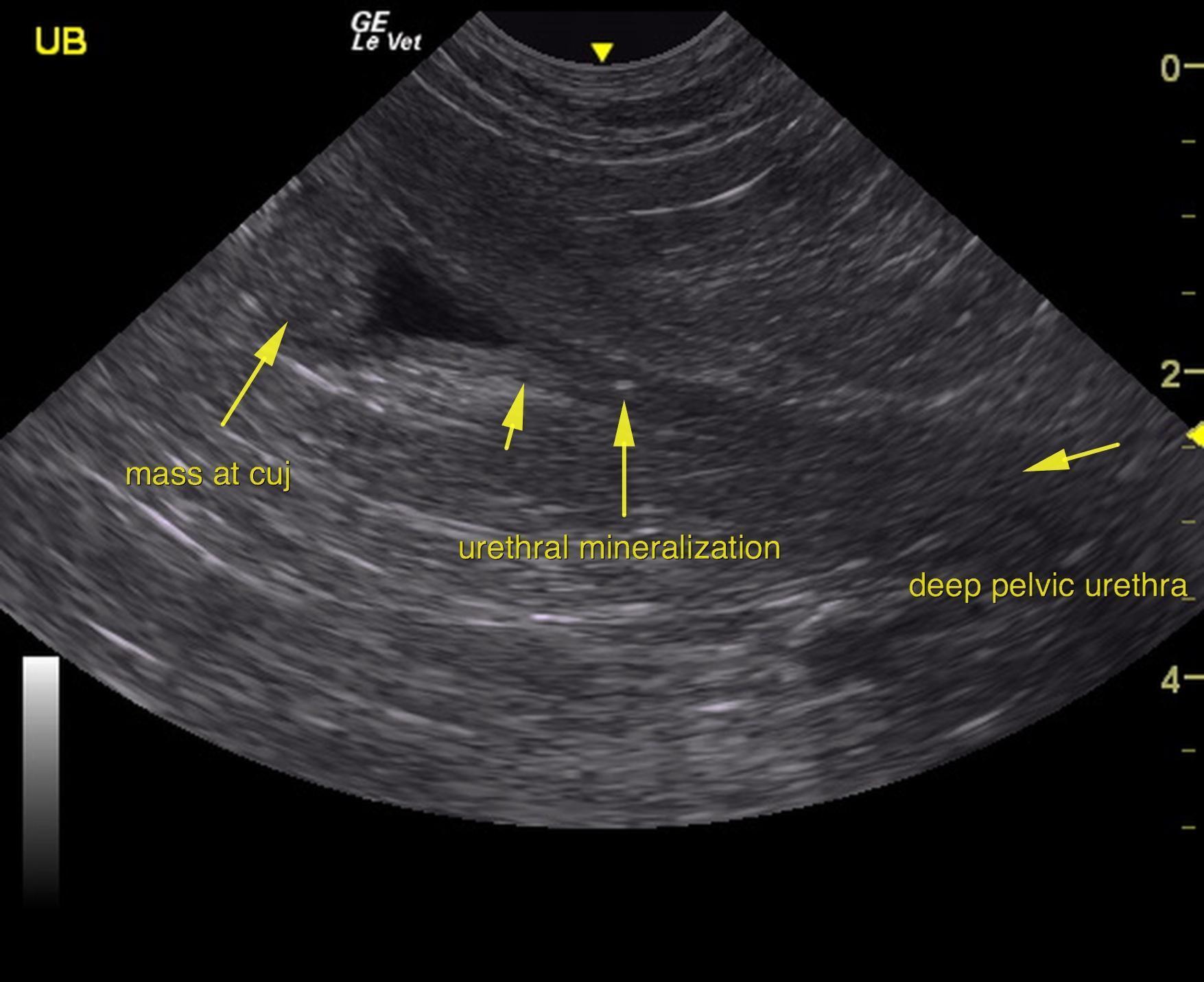
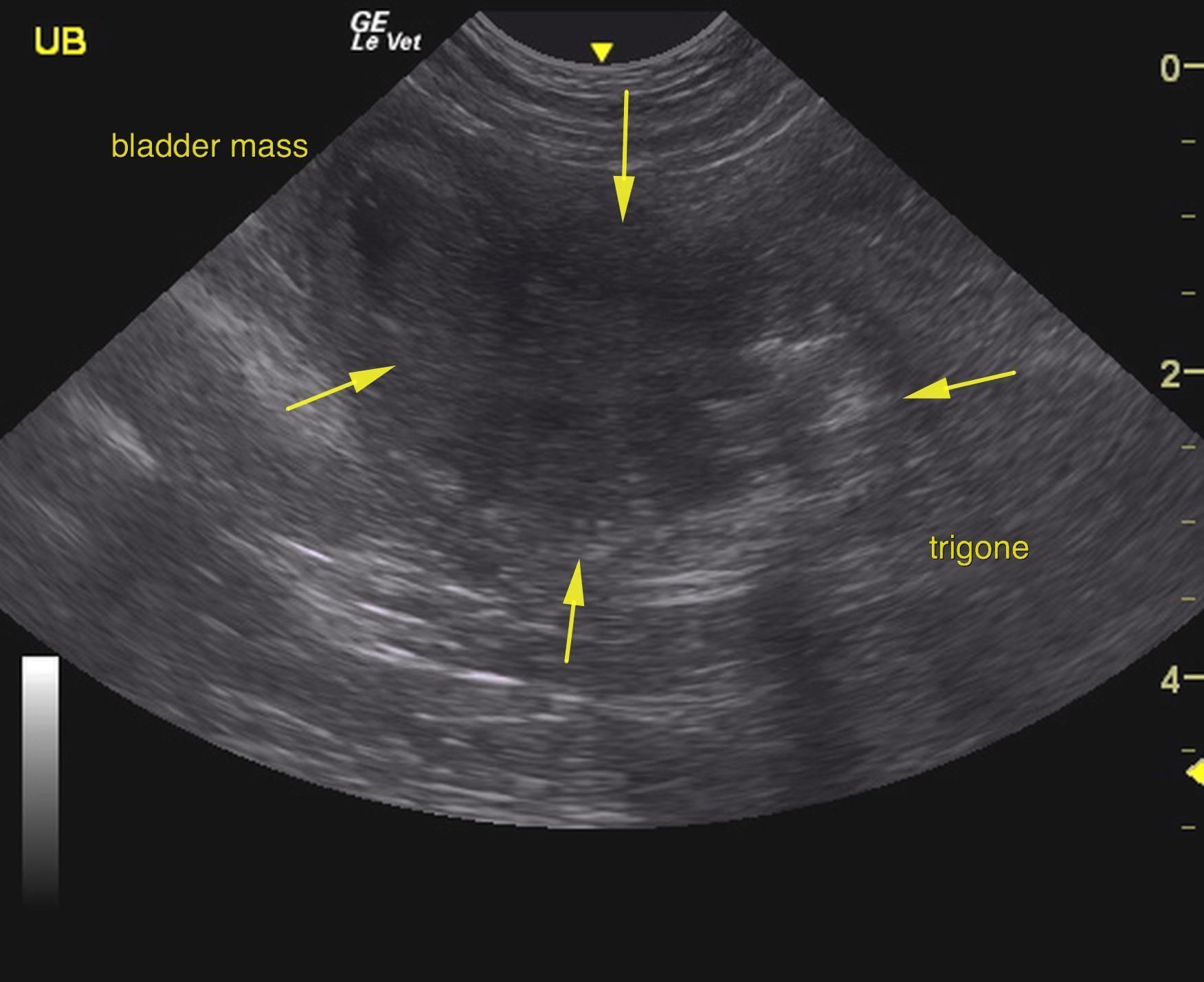
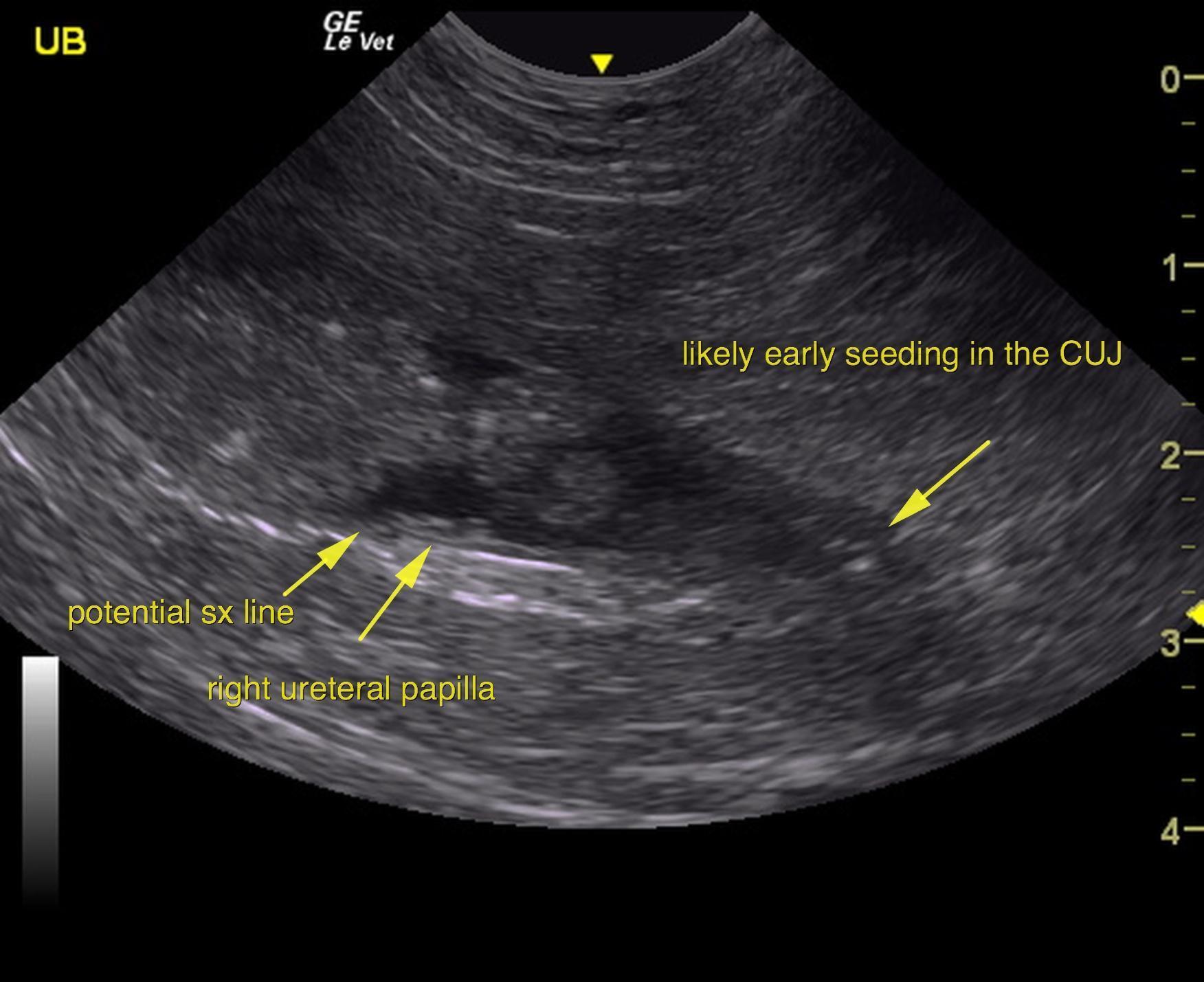
The urinary bladder presented a large, mineralizing mass that occupied the trigone and cystourethral junction as well as majority of the bladder. The mass measured approximately 4.0 x 3.0 cm and was moderately vascular. The mass appeared to be largely deriving from the ventral wall. Mineralizing pattern is consistent with transitional cell carcinoma. The mass does not appear resectable. Kissing lesion polyps were noted in the dorsal wall as well. Free calculi were also noted. The iliac trifurcation was unremarkable with no evidence of pathology or metastatic disease. Slight mineralization was noted in the urethra. Potential passing calculi or early seeding is possible. The pelvic urethra was imaged 3.0 cm beyond the cystourethral junction. Minor tissue thickening at the cystourethral junction may represent seeding caudally not allowing for complete surgical resection. The bladder reaches a point of 0.5 cm from the right ureteral papillae leaving minimal amount of space for surgical closure.
closure.
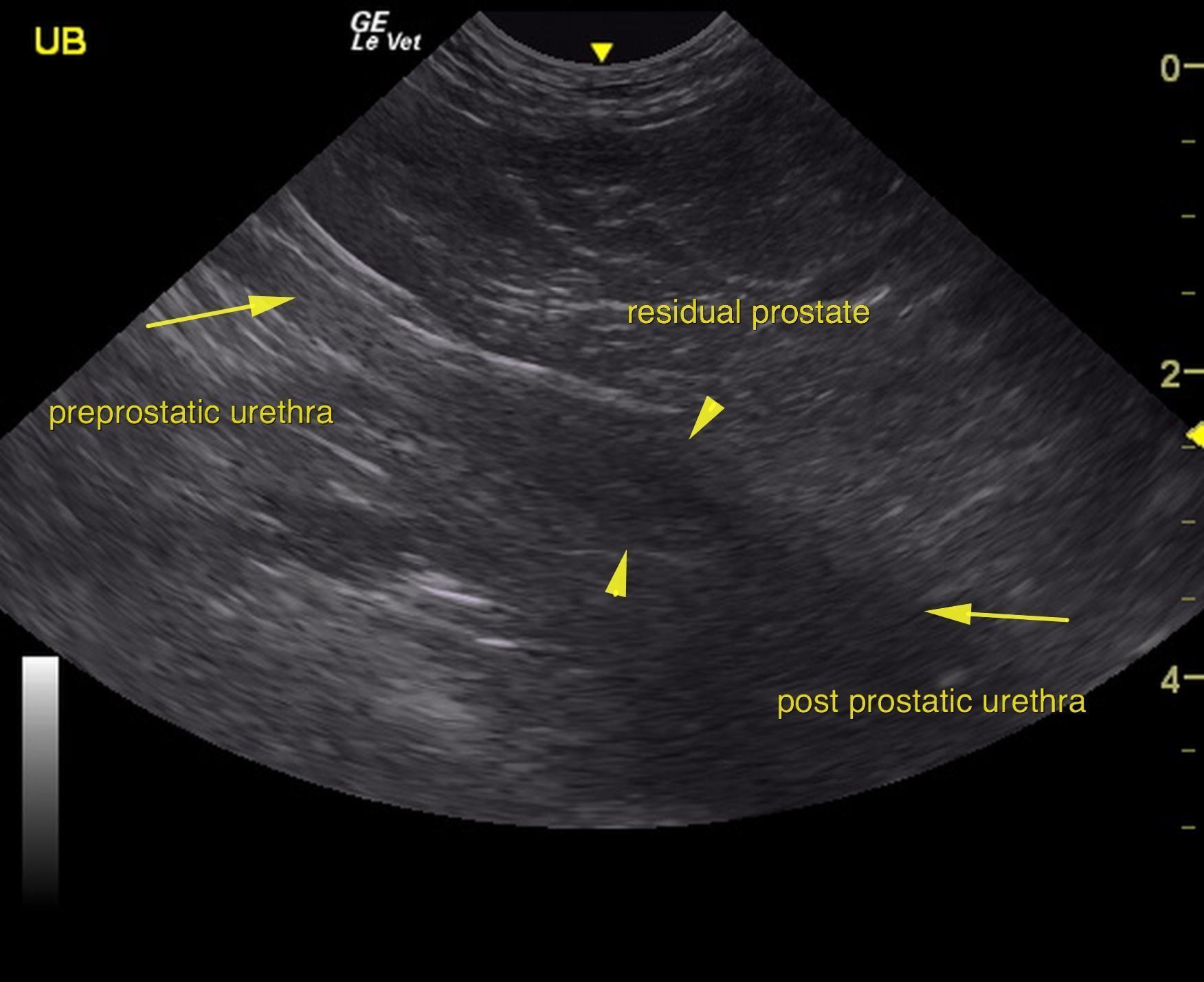
The residual prostate was uniform with no obvious seeding of the tumor.
The kidneys revealed largely normal size and structure, corticomedullary definition and ratio (cortex 1/3 of medulla) were essentially maintained with some age related loss of curvilinear patterns. The cortices presented largely uniform texture with some age related echogenic changes that are not likely of clinical significance at this time unless inflammatory sediment or proteinuria is present. Medullary echogenicity differed distinctly from that of the cortex and no evidence or dilation could be seen. The capsules were acceptably uniform for this age patient without dramatic irregularities. The right kidney measured 6.36 cm. The left kidney measured 5.2 cm.