Feb 2011 this 11-year-old MN Boxer was presented for cardiac arrhythmias that had been auscultated occasionally, and occasional PVCs noted on ECG. The dog was re-presented 7 months after being diagnosed with Boxer cardiomyopathy, that was been managed with 40 mg Sotalol BID. There had been two syncopal episodes in last week. Additional medication was 10 mg metoclopromide for nausea and 10 mg diazepam for anxiety. Abnormalities on clinical examination were a left side grade 2/6 systolic murmur.
Feb 2011 this 11-year-old MN Boxer was presented for cardiac arrhythmias that had been auscultated occasionally, and occasional PVCs noted on ECG. The dog was re-presented 7 months after being diagnosed with Boxer cardiomyopathy, that was been managed with 40 mg Sotalol BID. There had been two syncopal episodes in last week. Additional medication was 10 mg metoclopromide for nausea and 10 mg diazepam for anxiety. Abnormalities on clinical examination were a left side grade 2/6 systolic murmur. Urinalysis, thyroid profile, and CBC were all within normal limits; whereas elevated liver enzyme activity was evident on serum biochemistry.
Case Study
Advanced dilated cardiomyopathy (DCM in a 11 year old MN Boxer dog
Sonographic Differential Diagnosis
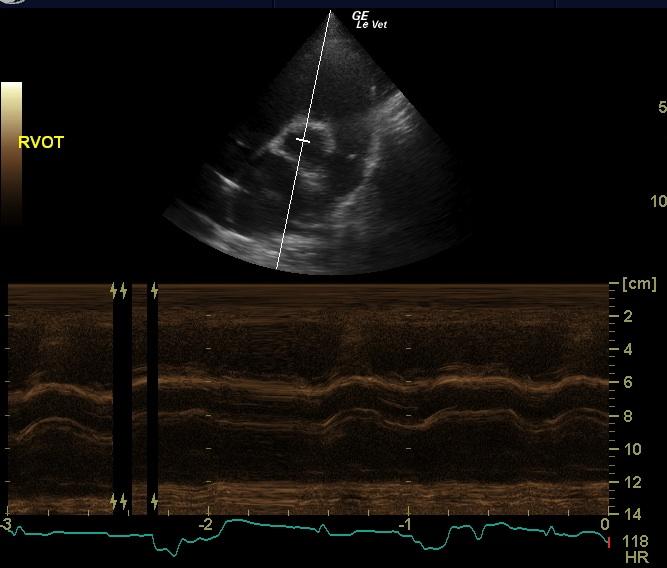
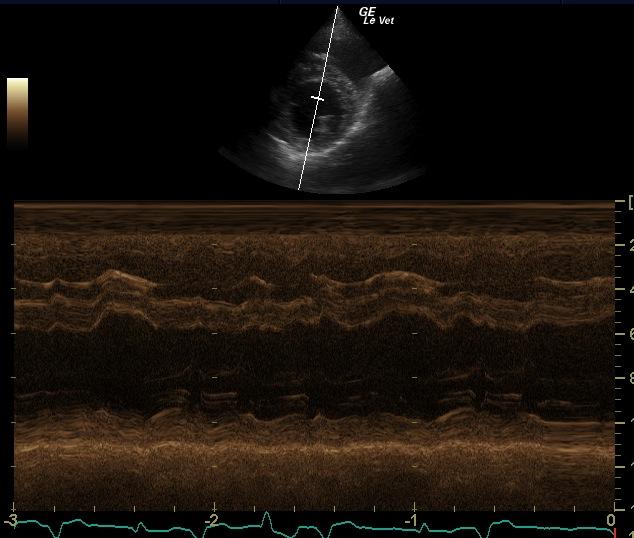
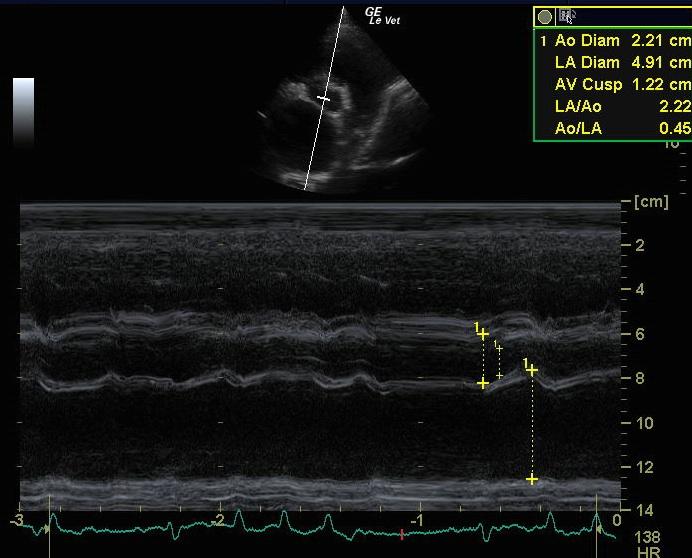
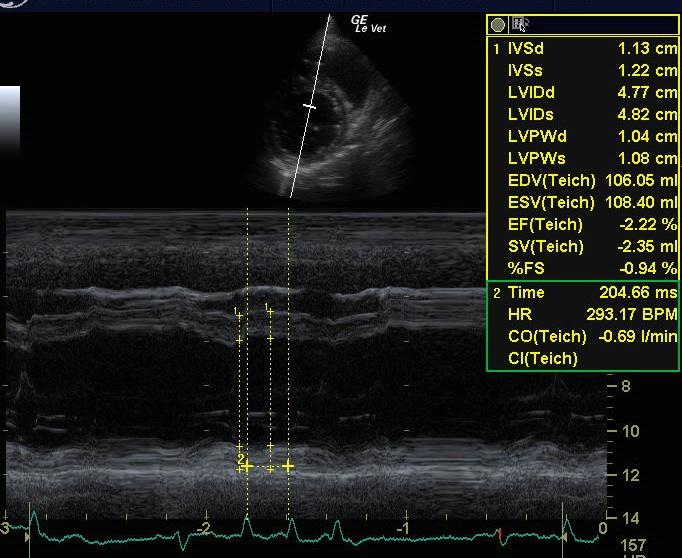
First presentation: The echocardiogram shows perhaps mild left ventricular dilation with reduced systolic function, normal left atrial size and frequent ventricular arrhythmia. The arrhythmia is likely due to arrhythmogenic right ventricular cardiomyopathy (ARVC, Boxer cardiomyopathy) but other systemic conditions such as pain, excitement, reduced perfusion or a splenic mass could also be playing a role. The arrhythmia would be relatively well tolerated as seen here but this does not rule out the presence of more significant arrhythmia at other times and puts the dog at some risk for sudden death. The condition has progressed since the previous exam with more significant left ventricular and atrial enlargement. The syncopal episodes may be due to more significant ventricular arrhythmia at other times but the structural changes are also likely playing a role. The atrial enlargement also puts the dog at risk for heart failure.
Image Interpretation
First presentation: The left atrium appears normal to slightly enlarged in size. The left ventricular cavity is normal to mildly dilated in diastole (4.5 cm) and mildly dilated in systole (3.4 cm) with a mildly depressed fractional shortening (24 %). The left ventricular walls are normal (1.1 cm septal wall and 1.1 cm free wall). There is mild mitral and trace tricuspid regurgitation on Doppler exam. The heart rate is measured at about 115 bpm and there are frequent, single and paired, multiform VPCs seen on an ECG run during the exam. Re-presentation: The left atrium is now moderately to markedly enlarged in size. The left ventricular cavity is moderately dilated in diastole (4.8 cm) and systole (4.0 cm) with a depressed fractional shortening (17 %) consistent with myocardial failure. The left ventricular walls are thinned (0.9 cm septal wall and 0.9 cm free wall). The right ventricle is mildly dilated and the right atrium is mildly to moderately enlarged in size. The main pulmonary artery appears enlarged in comparison to the aorta. There is moderate mitral and tricuspid regurgitation and the velocity of the tricuspid regurgitation is normal at 2.73 m/sec, consistent with normal pulmonary artery pressures. The heart rate is measured at 117 to 128 bpm and frequent VPCs with some runs of tachycardia and a bigeminal rhythm is seen on an ECG run during the exam.
DX
Outcome
An ECG is recommended to more fully define the heart rate and rhythm. Thoracic radiographs can also be considered to look for evidence of decompensation. Low dose lasix such as 25 mg PO SID to BID can be considered. Pimobendan at 7.5 mg PO BID is also recommended. If the ventricular arrhythmia were persistent despite this therapy, addition of mexiletine at 150 mg PO BID to TID can be considered to suppress it. If signs of heart failure develop, it may be better to taper the sotalol dose to 20 to 30 mg PO BID but if well tolerated, it can be continued at the present dose. Once the dog has improved with improvement in the ventricular arrhythmia, enalapril can be added at 10 mg PO SID and increased to 15 mg PO SID after a week if it is well tolerated. The heart rate can also be monitored to ensure it remains in the normal range and the ventricular arrhythmia improves. A renal profile is recommended a week after the final adjustments to the medications have been made to make sure they are well tolerated. The condition can be followed by thoracic radiographs or repeat echocardiogram every 6 months to monitor for signs of progression or decompensation. The resting heart rate can also be monitored to ensure it remains in the normal range.
Comments
At month 11 after first presentation, the dog continued to decline with episodes of collapse and was euthanized.
Clinical Differential Diagnosis
Cardiac – dilated cardiomyopathy, hypertrophic cardiomyopathy, myocarditis Splenic disease – neoplasia, hypersplenism, splenitis, infarction
Video
Patient Information
Clinical Signs
- Syncopal episodes
Exam Finding
- Arrhythmia
- Heart Murmur
Images
Blood Chemistry
- Elevated Liver Enzymes
Clinical Signs
- Syncopal episodes