An 11 year old FS DSH was presented for anorexia, decreased water consumption, and lethargy. There was the possibility of ingestion of a foreign body. Thrombocytopenia, lymphopenia and monocytosis were noted on the CBC. Blood chemistry showed hyperbilirubinemia, hyperphosphatemia, hypercholesterolemia and elevations of the ALT and AST enzyme activities. The urine was orange in color and had a cloudy appearance. The specific gravity was within normal limits, and bilirubinuria was present.
An 11 year old FS DSH was presented for anorexia, decreased water consumption, and lethargy. There was the possibility of ingestion of a foreign body. Thrombocytopenia, lymphopenia and monocytosis were noted on the CBC. Blood chemistry showed hyperbilirubinemia, hyperphosphatemia, hypercholesterolemia and elevations of the ALT and AST enzyme activities. The urine was orange in color and had a cloudy appearance. The specific gravity was within normal limits, and bilirubinuria was present.
Case Study
03_00166 Chloe S Common bile duct carcinoma
Sonographic Differential Diagnosis
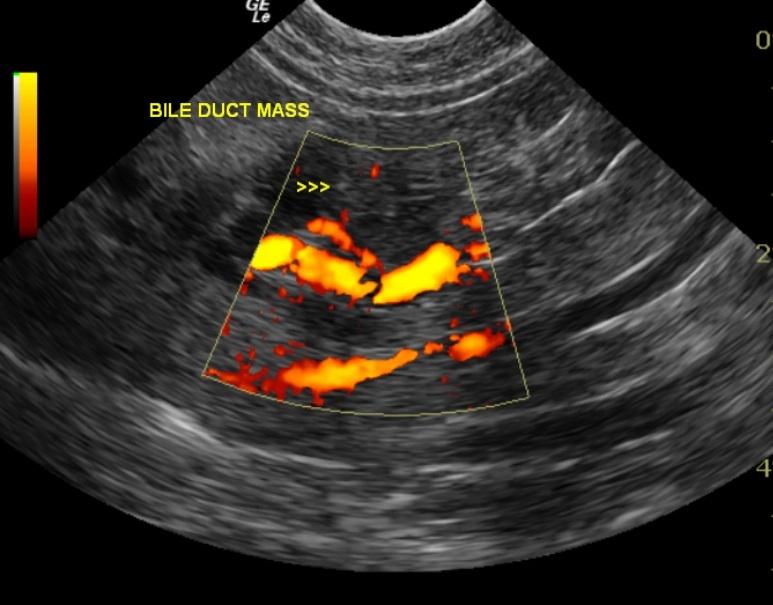
Suspected bile duct calculus with post hepatic bile duct obstruction vs an expansive bile duct neoplasm
Image Interpretation
The liver was examined and had homogeneous echotexture with smooth lobar structure. Portal vasculature, hepatic veins and biliary ducts appear within normal limits. No distinct focal nodules or lesions were noted. Porta hepatis structures appear within normal limits. There was a moderate amount of gallbladder sludge present within the gallbladder lumen. The common bile duct was tortuous and dilated to 0.49 cm. A single 0.94 cm, hyperechoic focus was located within the common bile duct. Approximately 2 cm distal to the gallbladder and was consistent with a small bile calculus or bile sludge.
DX
Outcome
The patient’s condition declined steadily following the initial ultrasound. The owner elected to treat the cat empirically for a biliary obstruction despite the fact that an expansive bile duct neoplasm was suspected. The owner allowed an ultrasound-guided biopsy performed postmortem. A diagnosis of a common bile duct carcinoma was made, in addition to the presence of a mild to moderate chronic cholangiohepatitis with associated diffuse hepatocellular swelling and mild cholestasis.
Clinical Differential Diagnosis
Cholangitis/cholangiohepatitis, cholelithiasis causing a biliary obstruction, pancreatitis with secondary cholestasis and/or cholangiohepatitis, Triaditis with an ascending bacterial infection, hepatic neoplasia (lymphoma, adenocarcinoma, leiomyoma, leiomyosarcoma, mast cell tumor,) biliary carcinoma, leptospirosis, toxoplasmosis and feline infectious peritonitis are less likely, but cannot be excluded depending upon the cat’s previous history/risk of exposure, etc.
Sampling
U/S- guided Tru-cut® biopsy obtained postmortem. A diagnosis of a common bile duct carcinoma was made, in addition to the presence of a mild to moderate chronic cholangiohepatitis with associated diffuse hepatocellular swelling and mild cholestasis.
Video
Media error: Format(s) not supported or source(s) not found
Download File: http://sonopath-videos.s3.amazonaws.com/sites/default/files/case_studies/videos/converted/03_00166_video_01_07292011012726.mp4?_=1Media error: Format(s) not supported or source(s) not found
Download File: http://sonopath-videos.s3.amazonaws.com/sites/default/files/case_studies/videos/converted/03_00166_video_02_07292011012738.mp4?_=2Patient Information
Clinical Signs
- Anorexia
- Concern for FB Ingestion
- Decreased Drinking
- Lethargy
Images

Blood Chemistry
- ALT (SGPT), High
- AST (SGOT), High
- Cholesterol, High
- Phosphorus, High
- Total Bilirubin, High
CBC
- Lymphocytes, Low
- Monocytes, High
- Platelet Count, Low
Clinical Signs
- Anorexia
- Concern for FB Ingestion
- Decreased Drinking
- Lethargy
Urinalysi
- Appearance Turbid
- Bilirubin Present
- Color Abnormal