This 7-year-old MN DSH presented for dysuria and a history of persistent UTI, which then progressed into episodes of vomiting and general malaise. The physical exam revealed a palpable mass in the cranial abdomen; this was confirmed by radiographs and was positioned caudal to the stomach. The CBC was normal. Blood chemistry was normal except for a mildly elevated globulin. A free catch urinalysis revealed a pH of 6.0, USG 1.032, cloudy appearance, moderate leukocytes, and 100+ protein. Epithelial cells and cocci bacteria were seen in the sediment.
This 7-year-old MN DSH presented for dysuria and a history of persistent UTI, which then progressed into episodes of vomiting and general malaise. The physical exam revealed a palpable mass in the cranial abdomen; this was confirmed by radiographs and was positioned caudal to the stomach. The CBC was normal. Blood chemistry was normal except for a mildly elevated globulin. A free catch urinalysis revealed a pH of 6.0, USG 1.032, cloudy appearance, moderate leukocytes, and 100+ protein. Epithelial cells and cocci bacteria were seen in the sediment.
Case Study
Marked pancreatitis, steatitis, and necrosis in a 7 year old MN DSH cat
Sonographic Differential Diagnosis
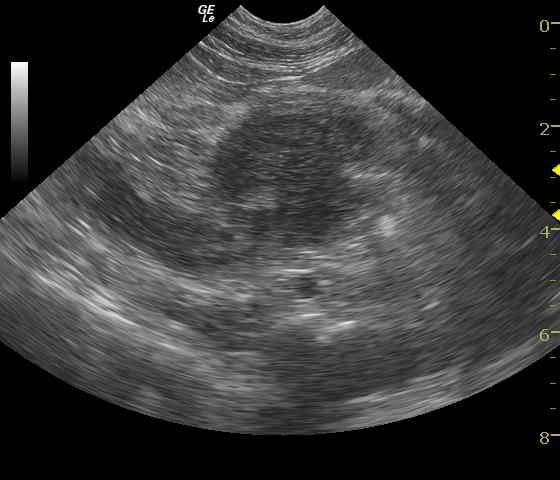
Suspect chronic pancreatitis with mild peripancreatic fibrosis, inflammation and adhesions with an accompanying avascular mass. Differentials for the mass include abscessing or necrotizing neoplasm or focal pancreatitis with sequestration.
Image Interpretation
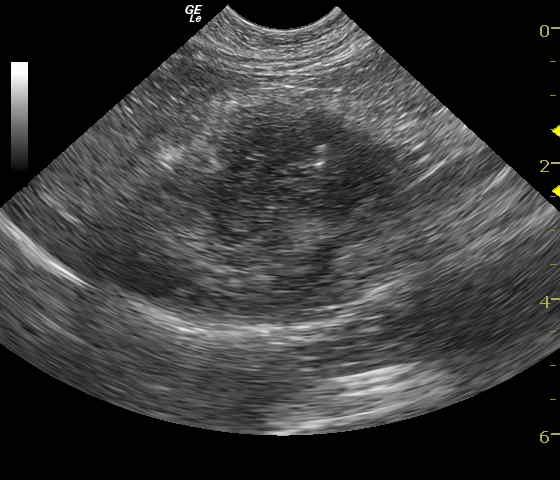
A well-circumscribed, hypoechoic mass positioned within the region of the body of the pancreas. The mesentery and omentum bordering the pancreas is mildly echogenic and may be adhered. Six-week post diagnosis (Videos 3 & 4) these videos demonstrate a reduction in size of the pancreatic necrosis by half but still largely void of blood flow indicated by lack of power Doppler signal.
DX
Outcome
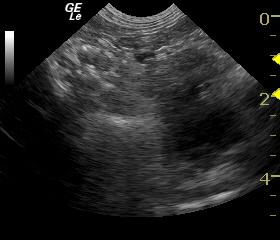
The patient responded well to IV fluid support, plasma expander therapy and intravenous antibiotics. Outpatient therapy included triple antibiotic therapy and supportive care. A single dose of dexamethazone was also administered. The patient thrived over the following 2 weeks when the follow-up sonogram was performed demonstrating a 50% reduction in the avascular hypoechoic pancreatic lesion. The patient was essentially asymptomatic at this time. Antibiotics were continued for an additional 3 weeks. Seven days after the antibiotics were stopped the patient presented again with lethargy and anorexia. Repeat ultrasound revealed that a splenic abscess had now formed (Image 3). The patient was again hospitalized and discharged 3 days later responding to enrofloxacin and D-methionine therapy.
Surgical biopsies were taken 2 months later (owner request) to further define the pathology. The patient was essentially stable at that time. Surgically-obtained histopathology 2 months post follow-up sonogram revealed the following:
1. Pancreatic nodular hyperplasia
2. Severe chronic lymphoplasmacytic cholangiohepatitis
3. Mild, chronic, lymphoplasmacytic enteritis
4. Moderate, chronic, fibrosing inflammation and splenic adhesion
5. Mild chronic, proliferative, mesenteric lymphadenopathy.
6. Mild, chronic, ulcerative, fibrosing cystitis.
The patient recovered uneventfully and was stable without medication 2 months post exploratory surgery.
Comments
This is typical histopathology of a triaditis cat. The pancreatic nodular hyperplasia would be consistent with sequelae from chronic pancreatitis.
Clinical Differential Diagnosis
Pancreatitis, neoplasia, IBD, infectious disease, UTI, and/or urolithiasis.
UA PH
UA PH
Sampling
22 gauge US-guided FNA was performed on various hypoechoic portions of the pancreas (Image 2 and Video 3). Cytology revealed marked pancreatitis, steatitis, and necrosis.
UA Specific Gravity Range
Video
Patient Information
Clinical Signs
- "Not Doing Right"
- Dysuria
- Vomiting
History
- UTI
Exam Finding
- Palpable mass
Images
Blood Chemistry
- Globulin, High
Clinical Signs
- "Not Doing Right"
- Dysuria
- Vomiting
Urinalysi
- Appearance Turbid
- Bacteria Present
- Protein Present
- WBCs Present