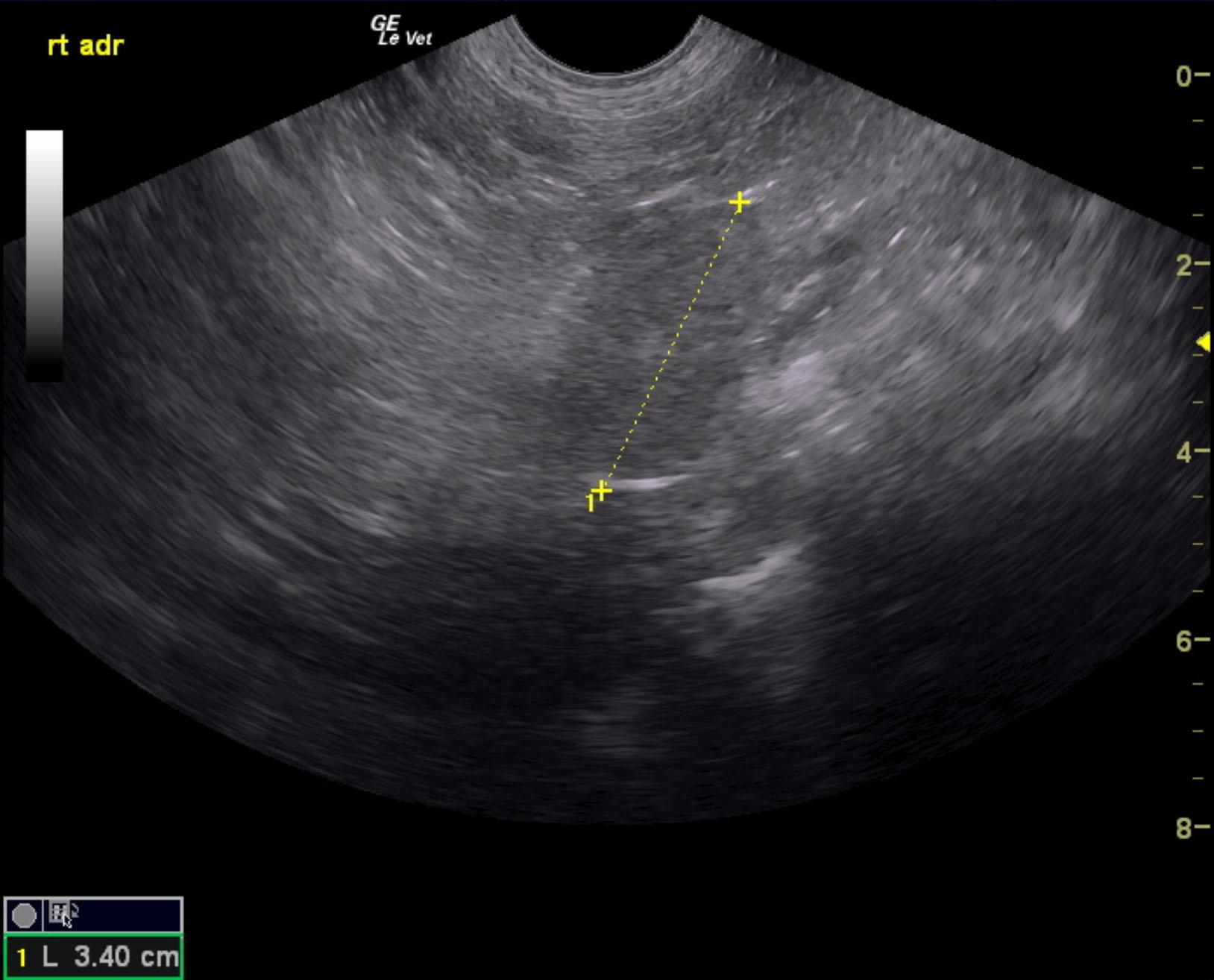
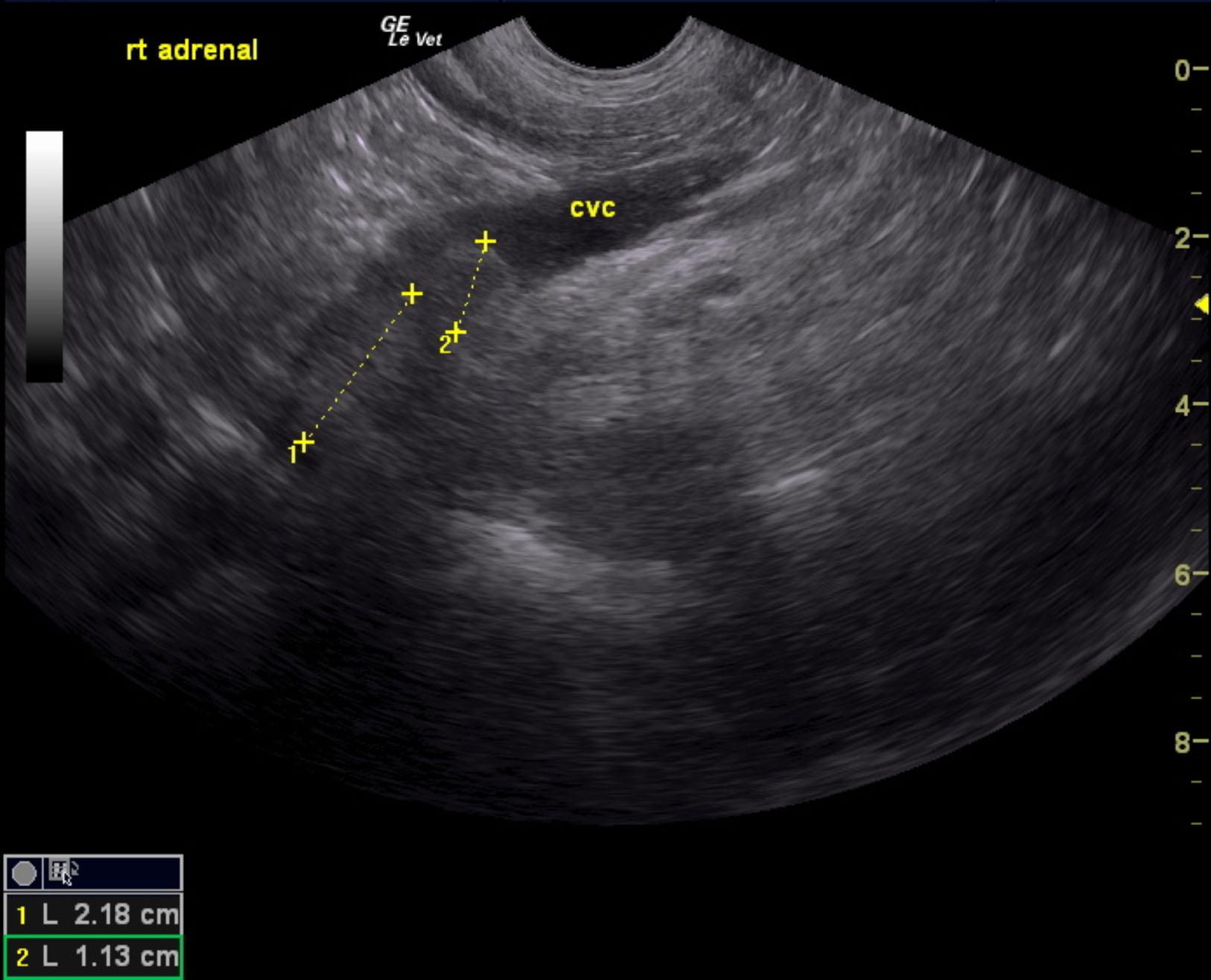
A 13-year-old SF Shepherd mix was presented for evaluation of episodic weakness, vomiting, and possible syncope. Abnormalities on serum biochemistry were elevated ALP activity (867) and creatinine (2.2).
A 13-year-old SF Shepherd mix was presented for evaluation of episodic weakness, vomiting, and possible syncope. Abnormalities on serum biochemistry were elevated ALP activity (867) and creatinine (2.2).